What is it?
The World Health Organization’s working definition of sexual health is “a state of physical, mental, and social well-being in relation to sexuality. It requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination, and violence.”[1]
Three aspects of sexual health — sexually transmitted diseases (STDs), dating violence, and unintended pregnancies — are each important indicators for the state of sexual health in San Francisco. Additionally, dating violence, among other risk factors, is associated with an increase in risk-taking sexual behaviors, an STD diagnosis, and unintended pregnancy.[2], [3]
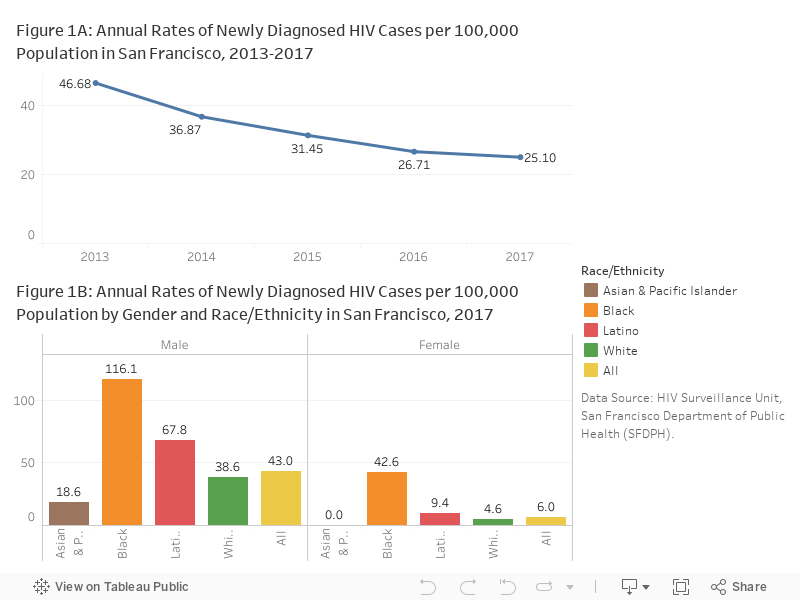
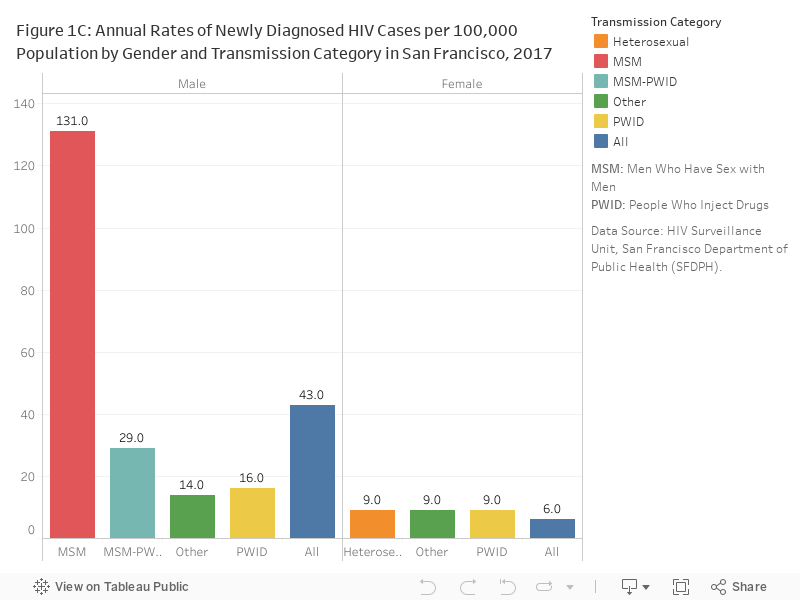
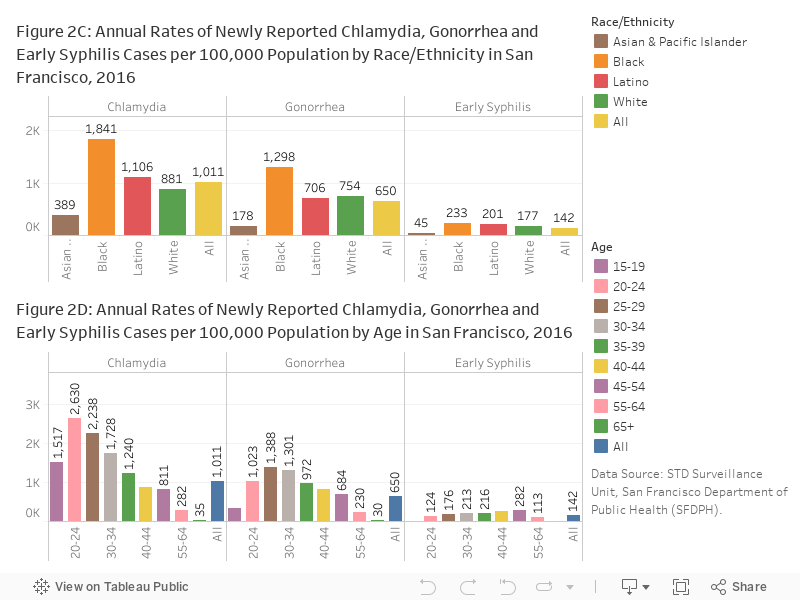
Chlamydia, gonorrhea, HIV, and syphilis are all examples of STDs. All STDs are preventable, and bacterial STDs such as chlamydia, gonorrhea, and syphilis are curable. Syphilis occurs in distinct stages, with early syphilis being subdivided into primary, secondary, and early latent syphilis. Early latent syphilis is when the STD is most contagious. Risk factors for acquiring an STD include being sexually active in communities with high rates of STDs, poverty and marginalization, limited access to health care, limited health care – seeking behavior, abuse of drugs and alcohol, stigma and secrecy around talking about sex and STDs, and early initiation of sexual intercourse.[3]
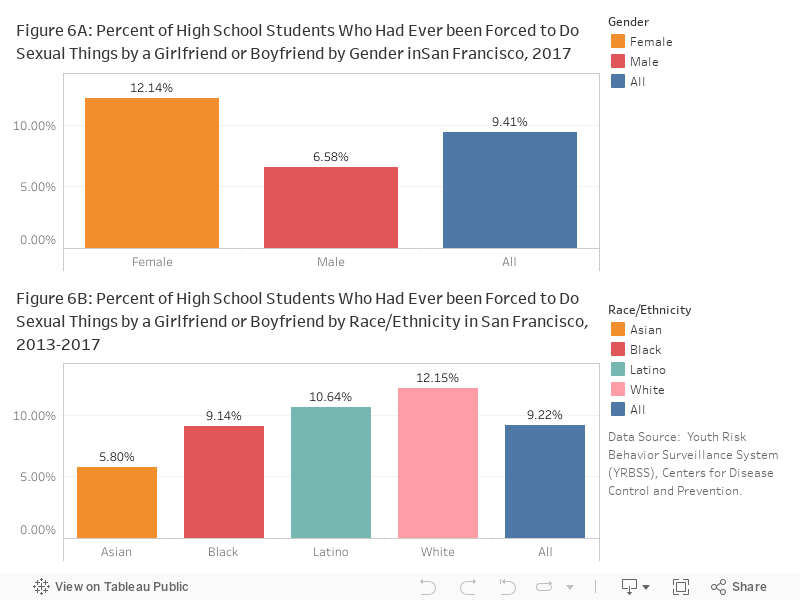
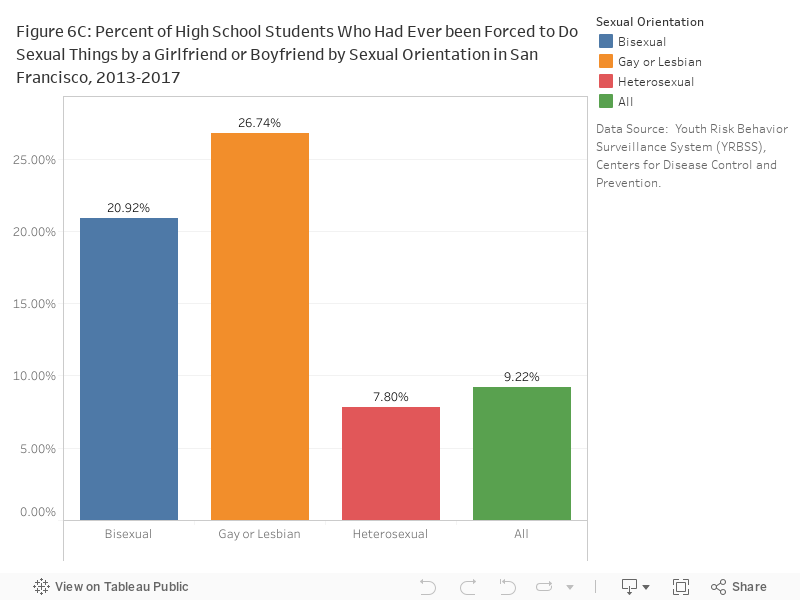
Dating violence is defined as physical, sexual, psychological, or emotional violence within a dating relationship.[4] In addition to lethal violence, abuse includes the intentional sabotaging of contraception, deliberately exposing someone to STDs, and forcing a woman into having unwanted pregnancies or abortions.[5] Risk factors for dating violence include the belief that dating violence is normal and acceptable, depression and other symptoms of trauma, aggression in other relationships, drug and alcohol abuse, engaging in early sexual activity and having multiple partners, having friends involved in dating violence, having conflicts with a partner, and experiencing violence in the home.
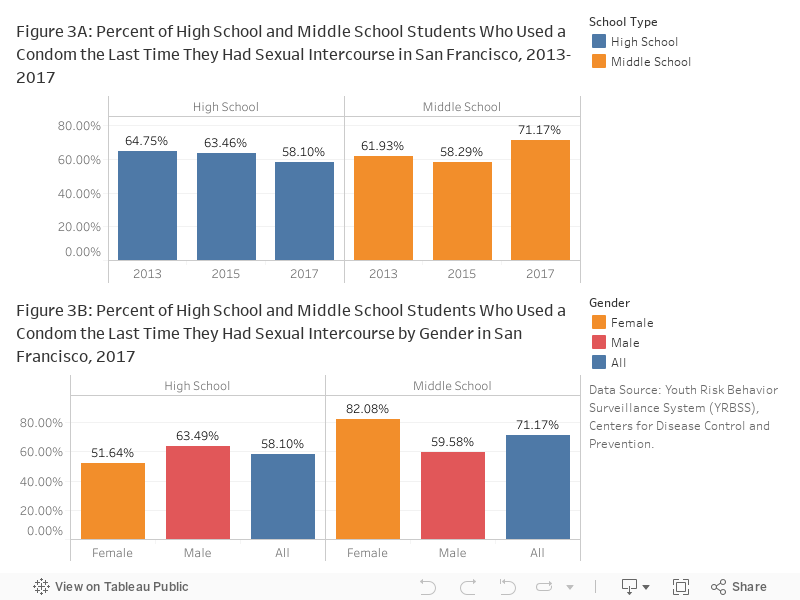
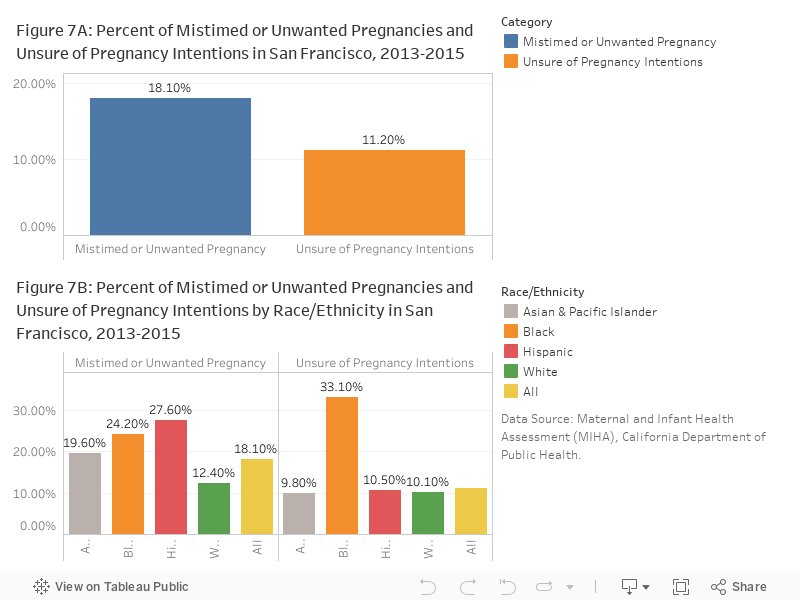
Unintended pregnancies are those that are mistimed, unplanned, or unwanted at the time of conception.[6] The rate of occurrence for unintended pregnancies varies according to a variety of factors, including maternal age, race/ethnicity, poverty, and education.[7] Some risk factors for unintended pregnancies are unavailability of contraception, failure to use contraception appropriately, and reproductive and sexual coercion.[8] The American Academy of Pediatrics (AAP) recommends long-acting reversible contraceptives (intrauterine devices (IUDs) or subdermal implants) as the first-line contraceptive choice for adolescents who do not choose abstinence.[9]
Why is it important for health?
Untreated STDs can lead to serious long-term health consequences, including reproductive health problems, fetal and perinatal health problems, cancer, and facilitated transmission of HIV. For example, chlamydia can damage a woman’s reproductive system and create pregnancy complications or even infertility.
Dating violence can have a negative effect on health throughout life. Victims of dating violence are more likely to experience symptoms of depression and anxiety. They might also engage in unhealthy behaviors, such as using tobacco, drugs, and alcohol, or inconsistent use of condoms and hormonal contraceptives. Dating violence is associated with unwanted pregnancy.[3] Teens who are victims of dating violence in high school are at higher risk for victimization later in life.[10], [11]
Unintended pregnancies are associated with many negative health and economic consequences. Negative outcomes that may occur for women during the unwanted pregnancy include delays in initiating prenatal care, reduced likelihood of breastfeeding, maternal depression, and increased risk of physical violence during pregnancy. Babies born under these circumstances often suffer from birth defects and low birth weight, as well as poor mental and physical health during childhood, and tend to have lower educational attainment and more behavioral issues in their teen years. The consequences are augmented for teen parents, who are less likely to graduate from high school and will over a lifetime earn significantly less income than those who delayed childbearing.[12] Unintended pregnancies also result in significant costs to the health system.[13]
What is the status in San Francisco?