Variables
- Salmonellosis
- Shigellosis
Enteric diseases can be caused by bacteria, parasites, or viruses, and can include a range of symptoms, such as diarrhea and vomiting. They are generally transmitted by consuming contaminated food or beverages or having direct contact with contaminated feces or vomit. In San Francisco, salmonellosis and shigellosis are two of the most common enteric diseases caused by bacteria. Other common enteric diseases are campylobacteriosis, shigatoxin-producing E. coli(STEC), hepatitis A, and vibriosis.[1] Although anyone can get an enteric infection, those age 50 and older and those with reduced immunity are at a greater risk for hospitalizations and death.[2] Safe food handling, frequent and careful handwashing with soap, as well as other hygiene measures can prevent salmonellosis, shigellosis and other enteric diseases.
Each year in the United States, Salmonella infections cause approximately 1.2 million illnesses, with 23,000 hospitalizations and 450 deaths.[3] It accounts for $365 million in direct medical costs each year.[4] Salmonella has been responsible for numerous multistate foodborne outbreaks and food recalls.[5] While E. coli infections have declined in the United States since 1997, salmonellosis incidence has not.[4] Healthy People 2020 (HP 2020) calls for reducing the incidence rate of infections caused by Salmonella species to 11.4 cases per 100,000 residents.[2]
Approximately 131,000 Shigella infections are estimated to occur each year in the United States, with 20% requiring hospitalizations.[6] Shigella is extremely infectious, with only a small amount of bacteria needed to cause disease.[7] Because the bacteria is easily transmitted from person to person and through sexual activity, outbreaks of shigellosis have occurred in the U.S. among different communities, such as the homeless/marginally housed and men who have sex with men.[7, 8] Antibiotic resistance is a growing concern, with an estimated 27,000 antibiotic resistant Shigellainfections in the United States each year.[9] Antibiotic-resistant shigellosis is harder to treat, can increase the cost of treatment, and can lengthen the duration of sickness, increasing the chances of spreading the disease.[9]
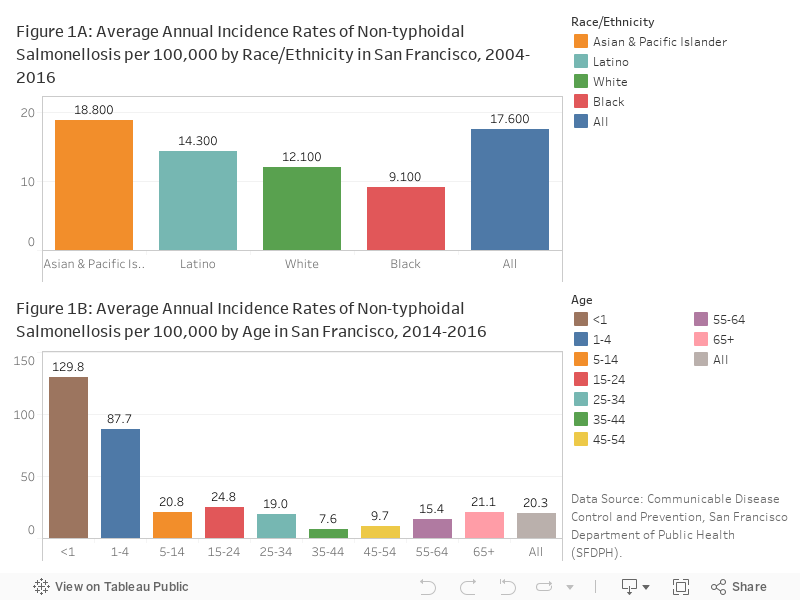
Salmonellosis:Salmonellosis incidence rates in San Francisco were consistently above the HP 2020 target of 11.4 cases per 100,000 population.Between 2014 and 2016, the average annual incidence of salmonellosis in San Francisco was 20.3 cases per 100,000 population. The rate of salmonellosis was the highest among Asians and Pacific Islanders (Figure 1B) and children under five years of age (Figure 1C).
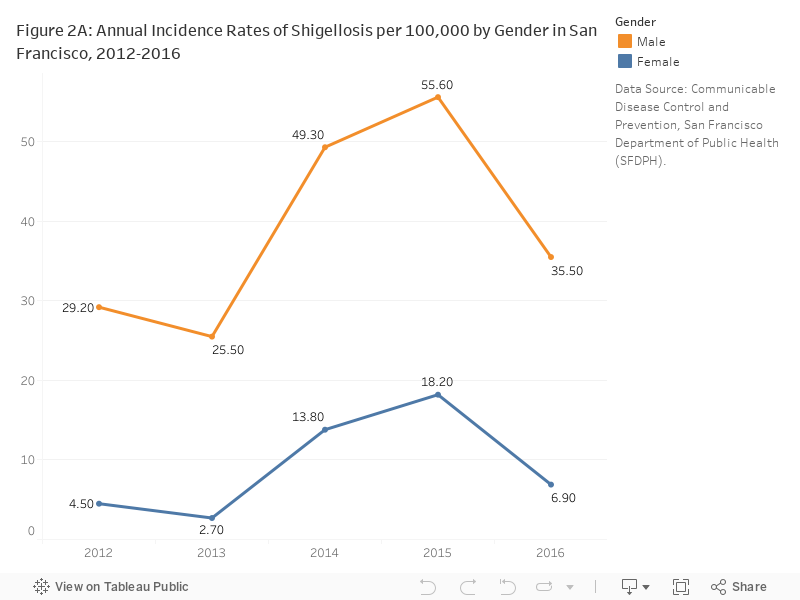
Shigellosis: Rates of shigellosis in San Francisco were consistently one of the highest in the state, with an incidence rate of 21.4 cases per 100,000 residents in 2016.[10,11] In 2014-15, rates of Shigellosis increased compared to the previous years due to several local outbreaks, including a citywide outbreak of ciprofloxacin-resistant shigellosis that disproportionately affected homeless and marginally housed individuals in San Francisco (Figure 2A). Generally, rates among men are significantly higher than women in San Francisco (Figure 2A). This is primarily attributed to sexual transmission among men who have sex with men.[12]
SFDPH Communicable Disease Control & Prevention, San Francisco Department of Public Health (SFDPH).
Data shown for a given year is by the date of report of the salmonellosis or shigellosis case to SFPDH. Data excludes Salmonella typhi which causes typhoid fever. Rates reported likely underestimate the burden of salmonellosis and shigellosis in San Francisco since most people do not go to the doctor when they get a diarrheal illness.
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
…few respondents to a survey,
…small population sizes, or
…small numbers of affected individuals.
Statistical instability indicates a lack of confidence in an estimates ability to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
1. Centers for Disease Control and Prevention, Enteric Disease Epidemiology Branch. https://www.cdc.gov/ncezid/dfwed/edeb/index.html
2. Office of Disease Prevention and Promotion, Food Safety. https://www.healthypeople.gov/2020/topics-objectives/topic/food-safety/objectives
3. Centers for Disease Control and Prevention, Salmonella. https://www.cdc.gov/salmonella/
4. Centers for Disease Control and Prevention, “Making Food Safer to Eat”. https://www.cdc.gov/vitalsigns/FoodSafety/index.html?s_cid=cs_074
5. Centers for Disease Control and Prevention, List of Selected Multistate Foodborne Outbreak Investigations. https://www.cdc.gov/foodsafety/outbreaks/multistate-outbreaks/outbreaks-list.html
6. National Institute of Allergy and Infectious Diseases, Shigellosis. https://www.niaid.nih.gov/diseases-conditions/shigellosis
7. Centers for Disease Control and Prevention, Shigellosis – Sources of Infection and Risk Factors. https://www.cdc.gov/shigella/infection-sources.html
8. Morbidity and Mortality Weekly Report (MMWR), “Importation and Domestic Transmission of Shigella sonnei Resistant to Ciprofloxacin – United States, May 2014-February 2015”. https://www.cdc.gov/shigella/infection-sources.html
9. Centers for Disease Control and Prevention, Antibiotic Resistance and Shigella Infections. https://www.cdc.gov/shigella/treatment/antibiotic-resistance-general.html
10. California Department of Public Health, “Yearly Summary of Selected General Communicable Diseases in California, 2001-2010”. https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/YearlySummaryReportsofSelectedGenCommDiseasesinCA2001-2010.pdf
11. California Department of Public Health, “Yearly Summary of Selected General Communicable Diseases in California, 2011-2016”. https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/YearlySummariesofSelectedCommDiseasesinCA2011-2016.pdf
12. Aragón, T J., et al. “Case-control study of shigellosis in San Francisco: the role of sexual transmission and HIV infection.” Clinical Infectious Diseases 44.3 (2007): 327-334.
