Variables
- Invasive Cancer Incidence
- Invasive Cancer Mortality
Cancer, a collection of more than 100 type of diseases, develops when human cells start to grow and spread out of control, which can result in death. Cancer can start almost anywhere in the human body and based on where the cancer starts, it is categorized by the organ or tissue type. When old cells become abnormal cells instead of dying, these extra cells may form a mass of tissue, called a tumor. Many cancers form tumors, for example, breast cancer, lung cancer, liver cancer, etc.; while some cancers, such as leukemia (cancer of the blood), do not form tumors.
Tumors can be malignant (cancerous) or benign (non-cancerous). Malignant tumors can spread and invade other tissues when the cancer cells travel through blood or lymph system to form new tumors. We use cancer staging 0-IV to describe the size and the extent of cancer: stage 0 (carcinoma in situ) indicates the cancer is non-invasive and the cancer cells are contained in one location; stage I-IV indicates the cancer is invasive [1]. Unlike malignant tumors, benign tumors do not spread or invade other tissues and when they get removed, they usually don’t come back. However, benign tumors can be life-threatening as well if they press on vital structures such as blood vessels or nerves [2].
Cancer is caused by gene mutations which affect the DNA that control the cell to function and perform normally. The majority of gene mutations occur after birth and they can be caused by environmental factors such as tobacco use, obesity, infectious organisms, chemicals, radiation, stress, etc.; and the remaining are due to inherited genetics [3]. Gene mutations can act together or independently to initiate or promote the development of cancer. Many years may pass between exposure to external factors and the detection of cancer. However, if cancers are detected and treated at their early stage, many can be cured or put into remission through treatments like surgery, chemotherapy and radiotherapy [4].
The American Cancer Society estimates that 1,688,780 new cases of cancer will be diagnosed and 600,920 people will die from cancer in the United States in 2017 [5]. The four most common cancers Nationwide, and in San Francisco, are breast, lung, prostate, and colorectal cancer, which account for 46% of all new cases and 45% of deaths [6]. Lung cancer is the leading cause of cancer deaths in both men and women; 80% of lung cancers deaths are attributable to cigarette smoking. Lung cancer is usually diagnosed at its late stages, which results in a low five-year survival rate-15% for men and 21% for women [7]. Breast cancer is the most common cancer and the second leading cause of cancer death among women. Early screening by mammography has been proven to be very helpful for reducing mortality [8]. Prostate cancer is the most common cancer among men and it can be cured if found in its early stages. Prostate-specific antigen testing is recommended for men beginning at age 50 [9]. Colorectal cancer, also known as colon cancer or rectal cancer, is the fourth most common type of cancer diagnosed in the United States. Deaths from colorectal cancer have decreased with the use of colonoscopies and fecal occult blood tests [10].
In San Francisco, liver cancer is the 5th common cause of cancer death and to a large extent is attributable to and hepatitis B and C infection. Liver Cancer disproportionally affects Asians which consist 35% of the population [11]. (See “hepatitis B and C” section for more details)
According to the American Cancer Society, there is strong evidence that an individual’s risk of developing cancer can be substantially reduced by healthy behavior [12]. They estimate that about 190,500, 32% of total cancer deaths in the United States in 2017, will be caused by tobacco use alone, and another third can be attributed to poor eating habits, overweight and obesity, and physical inactivity [13]. Moreover, cancer screening increase the chance of finding cancers in their early stages when they are most likely to be cured [14]. Promoting healthy behaviors can reduce or prevent much of the suffering and death caused by cancer.
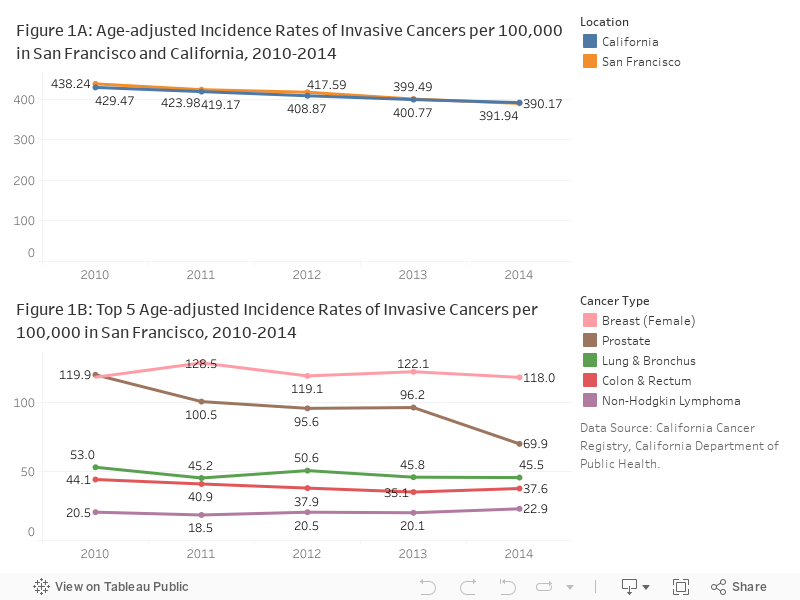
Invasive cancer incidence: Between 2010 and 2014, rates of invasive cancer per 100,000 population decreased from 438.24 to 390.17. Invasive Cancer rates in San Francisco are comparable to California rates (391.94 per 100,000 population in 2014) (Figure 1A).
The most common cancers in San Francisco were breast (females), prostate, lung & bronchus, colon & rectum and non-hodgkin lymphoma. Between 2010 and 2014, rates of prostate cancer decreased. Rates remained stable for all other types (Figure 1B).
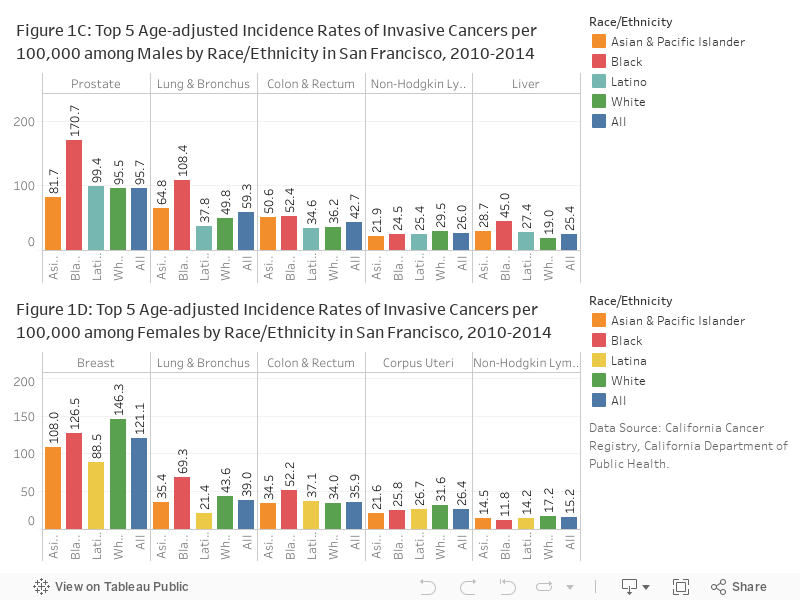
Ethnic variations are seen in cancer incidence rates. Among men, Black/African Americans had the highest incidence rates of prostate, lung& bronchus, colon & rectum and liver. Whites were most likely to have non-Hodgkin lymphoma (Figure 1C). Latino and Asian Pacific Islander women typically had lower incidences of all cancers. Incidence rates were the highest among Black/African American women for lung & bronchus and colon & rectum cancers and White women had the highest rates of breast, corpus uteri and non-Hodgkin Lymphoma cancer (Figure 1D).
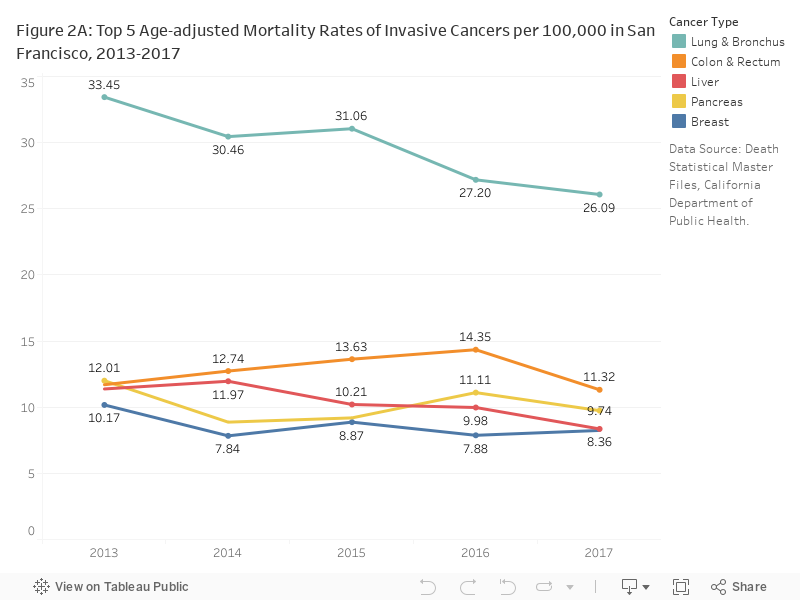
Invasive cancer mortality: Between 2013 and 2017, all-cause cancer death rates in San Francisco remained constant. The death rate for lung cancer, the top 1 cause of death, decreased from 33.45 to 26.09 per 100,000 population (Figure 2A). The leading types of cancer causing death were: lung & bronchus, colon & rectum, liver, pancreas and breast.
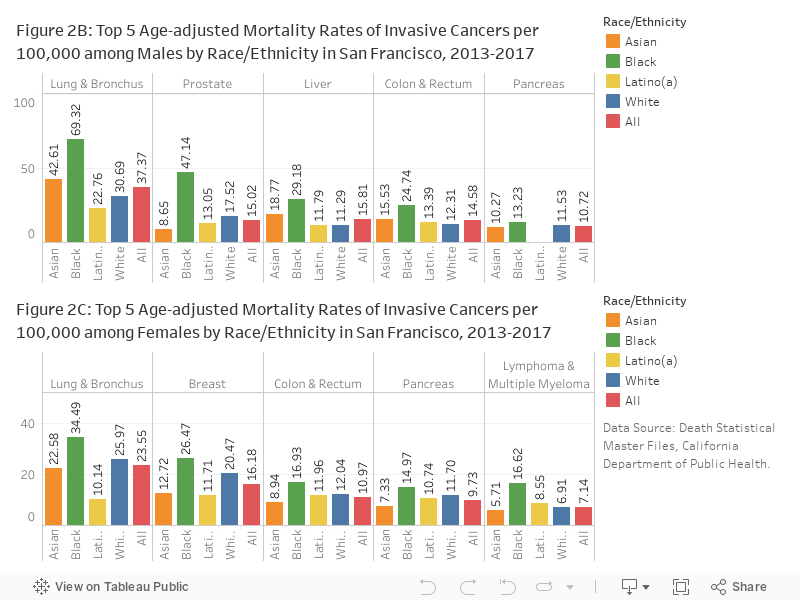
Cancer death rates for all of the leading cancers are highest among Black/African Americans. Among males, death rates due to lung & bronchus, prostate, liver, colon & rectum and pancreas were 85 percent to 213 percent higher for Black/African Americans than all males citywide (Figure 2B). Similarly, among females, rates of lung & bronchus, breast, colon & rectum, pancreas and lymphoma & multiple myeloma were 46 to 132 percent higher for Black/African Americans (Figure 2C).
CCRCAL: California Cancer Registry, California Department of Public Health.
CDPH: Death Statistical Master Files, California Department of Public Health.
Breast and prostate cancer: rates for gender-specific cancers were calculated using the population of only that specific gender. This makes the rates of gender-specific cancers more comparable to other types of cancer that consider the entire San Francisco population.
Invasive cancer: Not all cancer sites are reported due to small sample sizes (fewer than six cases).
Rates are per 100,000 and age-adjusted to the 2,000 US Standard Population (19 age groups —
Census P25-1130) standard. Incidence rates are dependent on frequency of cancer screening. If one gender, age group, or race/ethnicity is tested more often or thoroughly than another, that group will most likely report a higher incidence rate. This limitation could provide insight on the inconsistency between cancer incidence and mortality rates for specific sites when categorizing by race/ethnicity. For more information on Cancer Mortality statistics see the Mortality section of this Assessment.
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
…few respondents to a survey,
…small population sizes, or
…small numbers of affected individuals.
Statistical instability indicates a lack of confidence in an estimates ability to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
[1] National Cancer Institute. National cancer institute cancer staging. https://www.cancer.gov/about-cancer/diagnosis-staging/staging, 2015.
[2] National Cancer Institute. National cancer institute what is cancer. https://www.cancer.gov/about-cancer/understanding/what-is-cancer, 2015.
[3] National Cancer Institute. National cancer institute cancer genetics. https://www.cancer.gov/about-cancer/causes-prevention/genetics, 2017.
[4] National Cancer Institute. National cancer institute cancer treatment. https://www.cancer.gov/about-cancer/treatment/types, 2017.
[5] American Cancer Society. American cancer society estimated cancer new cases and deaths in 2017. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2017.html, 2017.
[6] American Cancer Society. American cancer society estimated number of new cases for the four major cancers in 2017. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/estimated-new-cases-for-the-four-major-cancers-by-sex-and-age-group-2017.pdf, 2017.
[7] American Cancer Society. American cancer society lung cancer. https://www.cancer.org/cancer/lung-cancer.html, 2017.
[8] American Cancer Society. American cancer society breast cancer. https://www.cancer.org/cancer/breast-cancer.html, 2017.
[9] American Cancer Society. American cancer society prostate cancer. https://www.cancer.org/cancer/prostate-cancer.html, 2017.
[10] American Cancer Society. American cancer society colorectal cancer. https://www.cancer.org/cancer/colon-rectal-cancer.html, 2017.
[11] Robert Hiatt and Alan Ashworth. San francisco cancer initiative. Technical report, UCSF Helen Diller Family Comprehensive Cancer Center, 2016.
[12] American Cancer Society. American cancer society stay healthy. https://www.cancer.org/healthy.html, 2017.
[13] American Cancer Society. American cancer society cancer facts & figures 2017. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdf, 2017.
[14] American Cancer Society. American cancer society cancer screening guidelines. https://www.cancer.org/healthy/find-cancer-early/cancer-screening-guidelines.html, 2017.
