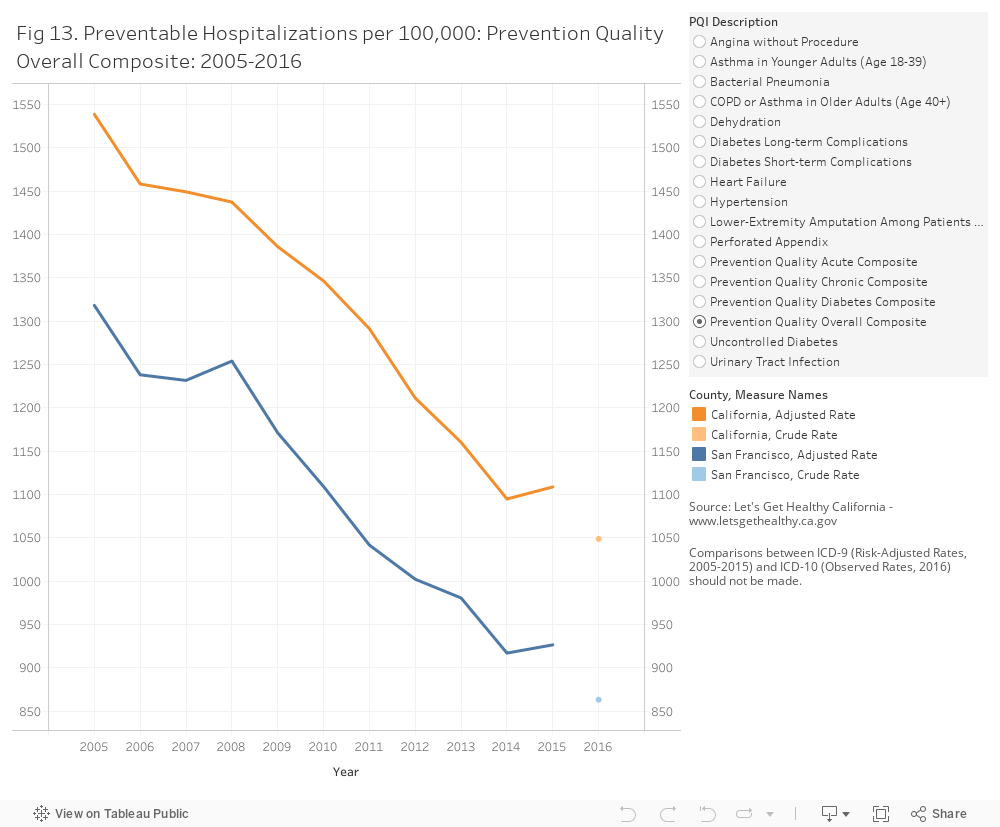
Preventable Hospitalizations: Preventable hospitalizations are those which can be prevented through access to high quality outpatient care. In 2016, the un-adjusted rate of preventable hospitalizations in San Francisco was 863 per 100,000 residents (Figure 13). Rates in San Francisco are consistently below that seen statewide. Since 2005, rates have been declining in San Francisco and Statewide .
What is currently being done in San Francisco to improve health?
Data Sources
ACS American Community Survey. https://www.census.gov/programs-surveys/acs/
CHIS UCLA Center for Health Policy Research, “California Health Interview Survey.” http://ask.chis.ucla.edu/main/default.asp
SFDPH San Francisco Department of Public Health
OSHPD Office of Statewide Health Planning and Development. http://www.oshpd.ca.gov/
Lets Get Healthy California. https://letsgethealthy.ca.gov/goals/redesigning-the-health-system/reducing-preventable-hospitalizations/
Methods and Limitations
Preventable Hospitalizations and Emergency Room Visits:
Hospitalization and ER rates measure the number of admissions or visits, not the number of residents who are hospitalized. Admissions records may include multiple admissions by the same person.
Preventable hospitalizations were analyzed by Let’s Get Health California. Data for 2015 are reported for nine months only due to a coding change from ICD-9 to ICD-10, which began October 1, 2015. ICD-9 comparisons across years should be made with caution since 2011-2014 results are based on 12 months of data, while 2015 rates are based on 9 months of data. Comparisons between ICD-9 (Risk-Adjusted Rates, 2005-2015) and ICD-10 (Observed Rates, 2016) should not be made.
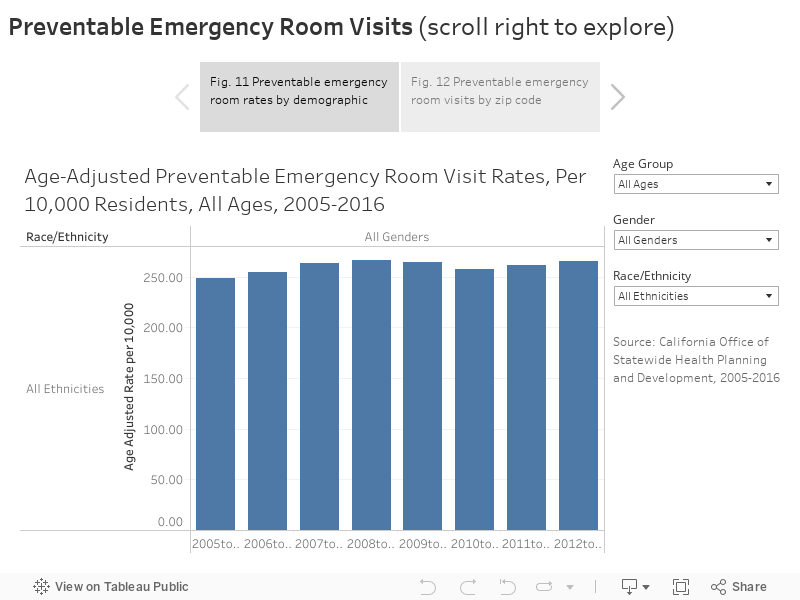
Preventable Emergency room visits were identified by searching the primary diagnosis field for ICD-9 and ICD-10 codes. ICD-9 codes associated with preventable emergency room visits were obtained from a report, “Statewide collaborative quality improvement project reducing avoidable emergency room visits, Final Remeasurement Report: January 1, 2010-December 31, 2010”, published by the California Department of Health Care Serivces, Medi-Cal Managed Care Division [6]. ICD-10 codes were obtained from a report published by the Oregon Health Authority, Ambulatory Care: Avoidable Emergency Department Visits [7] In October 2015, the diagnosis coding standard for Hospitalizations and Emergency Room visits was changed from ICD-9 to ICD-10. Caution should be used in comparing data (Pre 2015 and post 2015) using the two different standards.
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
…few respondents to a survey,
…small population sizes, or
…small numbers of affected individuals.
Statistical instability indicates a lack of confidence in an estimates ability to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
Areas of Vulnerability: Areas of Vulnerability (AOV) were created as a way to examine geographic data in relation to populations of concentrated socioeconomic disadvantage. The criteria to be designated as an AOV were:
1) Top 1/3rd of tracts for < 200% poverty or < 400% poverty & top 1/3rd for persons of color OR
2) Top 1/3rd of tracts for < 200% poverty or < 400% poverty & top 1/3rd for youth or seniors (65+) OR
3) Top 1/3rd of tracts for < 200% poverty or < 400% poverty & top 1/3rd for 2 other categories (unemployment, completing high school or less, limited English proficiency persons, linguistically isolated households, or disability)
Tracts that had unstable data for an indicator were automatically given zero credit for that indicator.
References
[1] 2020 Healthy People. Access to health services. http://www.healthypeople.gov/2020/topics-
objectives/topic/Access-to-Health-Services, 2017.
[2] U.S. Department of Health and Human Services. About the affordable care act.
http://www.hhs.gov/healthcare/rights/, 2017.
[3] San Francisco Department of Public Health. Healthy san francisco. http://healthysanfrancisco.org/.
[4] San Francisco Department of Public Health. San francisco health network. http://www.sfhealthnetwork.org.
[5] San Francisco Health Plan. http://www.sfhp.org/.
[6] California Department of Health Care Services. Statewide collaborative quality improvement project reducing
avoidable emergency room visits, final remeasurement report: January 1, 2010-december 31, 2010.
http://www.dhcs.ca.gov/dataandstats/reports/Documents/MMCD_Qual_Rpts/EQRO_QIPs/CA2011-
12_QIP_Coll_ER_Remeasure_Report.pdf, June 2012.
[7] Oregon Health Authority. Ambulatory care: Avoidable emergency department visits.
http://www.oregon.gov/oha/HPA/ANALYTICS/CCOData/Ambulatory%20Care%20-
%20Avoidable%20Emergency%20Dept%20Utilization%20-%202016.pdf, April 2017.