Variables
- PARK SCORE
- PUBLIC RECREATION FACILITIES
- PHYSICAL ACTIVITY IN CHILDCARE CENTERS
- WALKING AMONG ADULTS
- YOUTH PHYSICAL ACTIVITY
- YOUTH AEROBIC FITNESS
- STUDENTS MEETING STATE PHYSICAL FITNESS STANDARDS
Physical activity is defined as any bodily movement that requires energy expenditure. The Centers for Disease Control and Prevention (CDC) recommends that children and adolescents, age 5 to 17 years, should do at least 60 minutes of moderate -to-vigorous physical activity daily, while adults, age 18 years and above, should do at least 150 minutes of moderate-intensity physical activity, 75 minutes of vigorous-intensity physical activity, or an equivalent combination of moderate and vigorous activity throughout the week.[1] The National Association for Sport and Physical Education set physical activity guidelines for infants to children 5 years old at a minimum of 120 min of daily in the form of 60 min of structured activity and 60 minutes of unstructured activity.[2]
Regular physical activity can help people live longer, healthier lives. According to WHO, physical inactivity has been identified as the fourth-leading risk factor for mortality, causing an estimated 3.2 million deaths globally.[3] The CDC states that regular physical activity helps improve overall health and fitness, including aerobic capacity, performance (measured by the ability to run a mile and climb a minimum number of stairs), strength, endurance, and flexibility. Physical activity protects against many chronic health conditions including obesity, cardiovascular disease, type 2 diabetes, metabolic syndrome, and cancer (breast and colon). Through the release of serotonin, exercise can help reduce stress, anxiety, and depression.[4] Increased physical activity has also been linked to improved creativity.
Beyond physical and mental health, physical activity has been found to be vital to the success of students. It supports learning by improving concentration and cognitive functioning, and has been shown to have a positive influence on students’ academic performance.[5] California uses the FitnessGram® to assess physical fitness of 5th, 7th and 9th graders. On average, California students who achieve more fitness standards perform better on standardized tests.[6]
Despite health advantages of physical activity, a 2009 summary by the Robert Wood Johnson Active Living Research Program revealed that less than 50 percent of children and adolescents as well as less than 10 percent of adults in the U.S. achieve public health recommended goals of 30 to 60 minutes per day of moderate to vigorous physical activity on five or more days per week.[7]
The environments in which we live can have significant impact on our level of physical activity. Institutional policies and practices, living conditions, especially physical and social environments, and individual factors interact to promote or inhibit physical activity.[8–10] Land use and transportation policies determine the location and design of infrastructure and activities.[11] Neighborhood features such as parks, sidewalks, bicycle trails, recreational facilities, nearby shops, and public transportation stops promote leisurely physical activity, sports, and active transportation. [8,12-13] However, existence of infrastructure alone is insufficient. Barriers to use of facilities and physical activity include costs, poor access to facilities, and perceived unsafe environments.[13–15] Institutional policies, including those in the workplace and school and childcare, also affect health. Policies including transportation vouchers, on-location gyms, safe routes to school, recess, physical education, and after-hours availability of the school yard for play can boost physical activity among children and adults.[16] Additionally, social support is instrumental in starting and maintaining a physically active lifestyle. Persons who receive encouragement, support or companionship from family and friends are more likely to form positive views of physical activity and to begin and continue being physically active.[12-13,16-17] At the individual level, interest in and ability to do physical activity vary. Individuals may have physical or emotional blocks to doing physical activity. Examples include a lack of skills or confidence; a functional limitation associated with a disability, a chronic disease, or increased age; habits such as cigarette smoking or drinking alcohol; as well as a dislike for physical activity.[12,18-19] Additional personal barriers which are commonly cited are competing priorities, limited discretionary time and/or money, lacking availability to childcare, and a lack of culturally-appropriate activities.
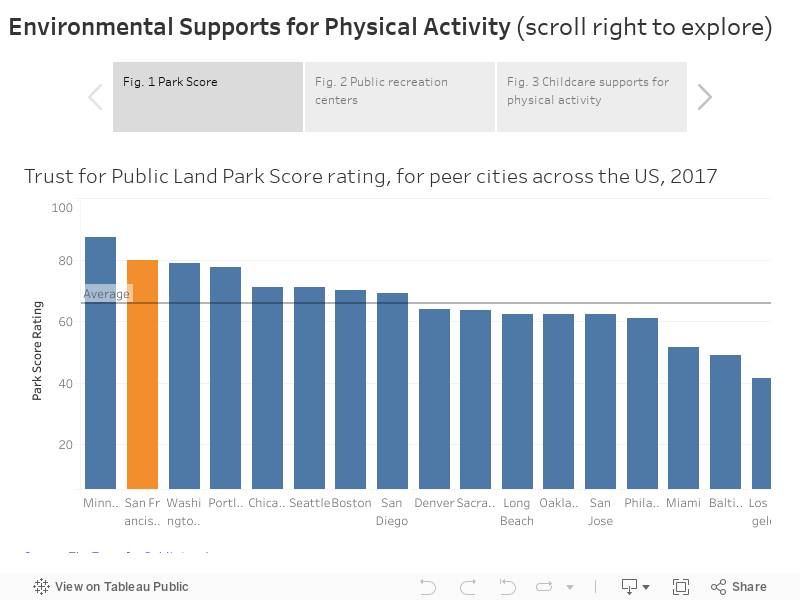
Park score: Among the 100 largest US cities, San Francisco ranks 5th on the Trust for Public Land’s Park Score (https://parkscore.tpl.org) (Figure 1). The Park Score methodology considers four components of park systems when calculating scores: 1) acreage (median park size + park acres as % of city acres), 2) investment (spending per resident), 3) amenities (availability of six key amenities per capita), and 4) access (percentage of the population living within a ten minute walk of a public park). San Francisco Scores best in the investment and access categories, scoring 40/40 for both. It falls short in terms of median park size and amenities (specifically playgrounds, recreation centers, restrooms, and splashpads).
Recreation facilities: Both the number of neighborhood parks near one’s residence and the types of amenities at the park (such as lighting, sports fields, etc.) can influence how much physical activity the population will engage in. Recreation facilities (defined as athletic fields, meeting spaces/activity centers, performance spaces, and recreational centers/pools) run by the San Francisco Recreation and Park Department (SFRPD) are geographically distributed in such a way that 95% of the population is within ½ mile of one (Figure 2). However, Treasure Island currently has no recreation facilities, and only 32% of Mission Bay and 41% of Financial District/South Beach residents are within ½ mile of a facility. Potrero Hill and western neighborhoods (including Sunset/Parkside, Inner Sunset, and Lakeshore) also have 10% or more of residents living more than a ½ mile away from a recreation facility.
Physical activity in child care centers: The San Francisco Department of Public Health’s Child Care Health Program works with child care providers to support them in implementing healthy policies in their facilities. Among those policies are 1) being active 90+ minutes/day, 2) no visible television, 3) physical activity posters, 4) active staff play with children, and 5) using a physical activity curriculum. Physical activity policy and practices in child care centers influence how much time young children spend doing physical activity. Between 2012-2017, there was an increase and then a decrease in the percent of target facilities where children were active for 90 or more minutes per day (Figure 3). At the same time, there was a steady increase in the percent of centers with no visible televisions. No discernible trends were present for other measures.
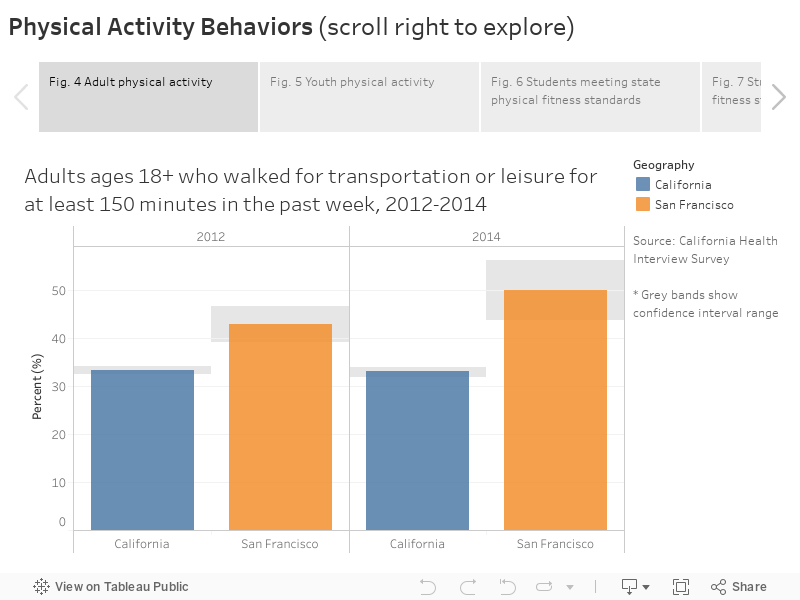
Adult physical activity: Walking or biking for utilitarian trips is an opportunity to incorporate routine physical activity into daily living. In San Francisco, 50% of adults age 18 and older reporting walking for transportation or leisure for at least 150 minutes in one week in 2014 (Figure 4). That is significantly higher than the 33% of adults statewide who walked for at least 150 minutes.
Youth physical activity: The Youth Risk Behavior Survey is conducted by the CDC and deployed in middle and high schools. Between 2009/11 and 2015/17 survey periods the percentage of middle school youth who reported meeting physical activity guidelines increased from 25% to 33% (Figure 5). No significant time trend was apparent for high school students or for the percentage of youth who played on a sports team in the past year for either age group. It is notable that the percentage of youth who report being active 60+ minutes per day each day of the week declines significantly between middle and high school (from 33% to 17%)
By sex, middle and high school aged females are significantly less likely to report being active on all days of the week compared to boys. There are no significant differences by sex in sports participation. The trend of middle school youth becoming more active is present in both males and females. By ethnicity, a greater percentage of White middle school youth are physically active compared to Chinese and Latino/a youth. A greater percentage of White middle school students also played on sports teams compared to Chinese and Latino/a students. Among high school students, White students were significantly more likely to be active between 2009-2015. White high school students were also more likely to play on a sports team compared to Chinese students in the 2009-2011 survey period. By sexual orientation, a lower percent of high school students who identified as bisexual were physically active than heterosexual students between 2013-2017.
Youth physical fitness: The California State Board of Education uses the standardized FitnessGram® to test students in grades 5, 7, and 9. The FitnessGram® defines Healthy Fitness Zones (HFZ) in six areas: aerobic capacity, flexibility, abdominal strength and endurance, upper body strength and endurance, trunk extensor strength and flexibility, and body composition. Students’ scores fall either within or outside of each HFZ, and children whose scores are within five or six HFZ are considered physically fit. Over time, the overall proportion of students scoring within five or six healthy fitness zones has remained relatively stagnant, with more than one-third of both 7th and 9th graders not physically fit (Figure 6). The proportion of students meeting this standard increases with age, and is higher for females than males. Children from economically disadvantaged households also perform worse than students from families who are not economically disadvantaged. Overall, San Francisco students perform worse than California students overall. While over 60% of Asian and White 9th grade students score within five or six zones, less than 40% of Black/African American, Latino, and Pacific Islander 9th grade students do the same (Figure 7).
One of the most potent measures of physical fitness from the FitnessGram® test is aerobic capacity, because of its relationship to cardiovascular and metabolic health. In San Francisco about 70% of 5th and 7th graders meet the standard for aerobic capacity (Figure 8). About 60% of high school students meet the standard. When examined by income, the percentage of students identified as not economically disadvantaged who met the aerobic standard was more than 10 percentage points higher than those identified as economically disadvantaged. By ethnicity, around 80% of White and Asian students meet aerobic standards in 5th and 7th grade while only 50-65% of Black and Latino/a students do the same (Figure 9). In 9th grade those rates for White and Asian students drop to around 70%, while for Black and Latino/a students they drop to around 40%.
TPL Trust for Public Land. https://parkscore.tpl.org/
SFRPD San Francisco Recreation and Parks Department. https://data.sfgov.org/Culture-and-Recreation/Recreation-and-Parks-Facilities/xvq2-rjrk
SFDPH San Francisco Department of Public Health. https://www.sfdph.org/dph/comupg/oprograms/MCH/CCHP.asp
CHIS California Health Interview Survey. http://askchisne.ucla.edu
YRBS Youth Risk Behavioral Surveillance System. http://www.cdc.gov/healthyyouth/data/yrbs/index.htm
CDE The California Department of Education, FitnessGram® physical fitness test. http://dq.cde.ca.gov/dataquest/
Recreation facilities: Recreation facilities run by the San Francisco Recreation and Park Department (SFRPD) that were included in this analysis include the following categories: performance spaces, meeting/activity centers, recreation centers/pools, and athletic fields.
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
Statistical instability indicates a lack of confidence in an estimate’s ability to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
[1] Centers for Disease Control and Prevention, “Physical Activity Guidelines,” Centers for Disease Control and Prevention. [Online]. Available: https://www.cdc.gov/cancer/dcpc/prevention/policies_practices/physical_activity/guidelines.htm. [Accessed: 07-Sep-2018].
[2] N. A. for Sport and P. Education (NASPE), Active Start: A statement of physical activity guidelines for children from birth to age 5. (2nd ed.). American Alliance for Health, Physical Education, Recreation, and Dance, 2009.
[3] World Health Organization (WHO), “Physical activity, Fact sheet No. 385, updated January 2015,” 2015.
[4] Robert Wood Johnson Foundation, “Active Education: Growing Evidence on Physical Activity and Academic Performance. 2015,” Robert Wood Johnson Foundation, 2015.
[5] C. E. Basch, “Physical activity and the achievement gap among urban minority youth.,” The Journal of school health, vol. 81, no. 10, pp. 626–634, Oct. 2011.
[6] G. Green, J. Henry, and J. Power, “Physical Fitness Disparities in California School Districts: A Practicum Issue Briefer for The City Project,” USC Price School of Public Policy, May 2015.
[7] Active Living Research Program, “Active Transportation: Making the Link from Transportation to Physical Activity and Obesity,” Active Living Research Program, 2009.
[8] Transportation Research Board, Does the Built Environment Influence Physical Activity? Washington, D.C.: National Academies Press, 2005.
[9] J. F. Sallis and M. F. Hovell, “Determinants of exercise behavior.,” Exercise and sport sciences reviews, vol. 18, no. 1, pp. 307–330, 1990.
[10] N. E. Sherwood and R. W. Jeffery, “The behavioral determinants of exercise: implications for physical activity interventions,” Annual review of nutrition, vol. 20, no. 1, pp. 21–44, 2000.
[11] E. S. L Parker AC Burns, Ed., “Local Government Actions to Prevent Childhood Obesity,” Washington (DC): National Academies Press (US), 2009.
[12] C. for D. Control and Prevention, Barriers to Physical Activity. 2016.
[13] S. Allender, G. Cowburn, and C. Foster, “Understanding participation in sport and physical activity among children and adults: a review of qualitative studies,” Health education research, vol. 21, no. 6, pp. 826–835, 2006.
[14] V. Rangul, T. L. Holmen, A. Bauman, G. H. Bratberg, N. Kurtze, and K. Midthjell, “Factors predicting changes in physical activity through adolescence: the Young-HUNT Study, Norway.,” The Journal of adolescent health : official publication of the Society for Adolescent Medicine, vol. 48, no. 6, pp. 616–624, Jun. 2011.
[15] V. Seefeldt, R. M. Malina, and M. A. Clark, “Factors affecting levels of physical activity in adults,” Sports Medicine, vol. 32, no. 3, pp. 143–168, 2002.
[16] A. C. Lindsay, M. L. Greaney, S. F. Wallington, T. Mesa, and C. F. Salas, “A review of early influences on physical activity and sedentary behaviors of preschool-age children in high-income countries,” Journal for Specialists in Pediatric Nursing, 2017.
[17] S. J. Chung, A. L. Ersig, and A. M. McCarthy, “The Influence of Peers on Diet and Exercise Among Adolescents: A Systematic Review,” Journal of Pediatric Nursing, vol. 36, pp. 44–56, 2017.
[18] S. Yazdani, C. T. Yee, and P. J. Chung, “Factors predicting physical activity among children with special needs.,” Preventing chronic disease, vol. 10, p. E119, Jul. 2013.
[19] K. Hesketh, R. Lakshman, and E. Sluijs, “Barriers and facilitators to young children’s physical activity and sedentary behaviour: a systematic review and synthesis of qualitative literature,” Obesity Reviews, 2017.
[20] California Department of Education, ARTICLE 3. Courses of Study, Grades 7 to 12, vol. Sections 51222-51223. 1976.
[21] C. G. M Szeto, “Shape Up SF PE Advocates: Recommendations to increase physical activity during the school day.,” Shape Up San Francisco, 2011.
