Variables
- Current Cigarette Smokers among Adults
- Smoking among High School and Middle School Students
- Smoking among Pregnant Women
- Tobacco Permits and Sales
Tobacco products are made entirely or partly of leaf tobacco as raw material, and are intended to
be smoked, inhaled, chewed, or sniffed. All of these products contain nicotine, a highly addictive psychoactive ingredient.
Electronic cigarettes (e-cigs or e-cigarettes) are electronic nicotine delivery devices that simulate tobacco smoking. These personal use products produce an aerosol containing a mixture of chemicals that may include nicotine. They usually contain any of over 7,000 flavors to modify the use experience.
Menthol cigarettes, flavored little cigars, cigarillos, or blunt wraps are combustible tobacco products that feature prominent flavors as additives to the leaf tobacco.
Tobacco, the number one preventable cause of the death, claims nearly half a million lives a year in the United States and estimates have shown that 18% of all US deaths could have been avoided if not for tobacco products.[1, 2] Tobacco products are cancer-causing and contribute to nearly every type of cancer. Cigarette smoking increases the risk of heart disease; chronic obstructive pulmonary disease; acute respiratory illness; stroke; and cancers of the lung, larynx, oral cavity, pharynx, pancreas, breast, and cervix.[1, 3, 4]
There is growing concern that flavored tobacco products, particularly menthol cigarettes, serve as easier starter products, may prove more addictive than non-flavored products, and have been shown to be harder to quit.[1, 3, 5] Flavored products stand in the way of tobacco control efforts, and may encourage youth use as well as co-use of cannabis. [6]
Numerous factors affect the decision to start smoking or use other tobacco products, including some individual characteristics, such as stress and low self-esteem, but also social characteristics, such as having friends and family who smoke. Tobacco industry targeting commences early, as tobacco addiction starts early in the developmental period, with over 90% of adult tobacco users having started smoking prior to age 18.[7] Adolescents who lack college plans or whose parents are not college educated are also more likely to smoke. Tobacco advertising can also foster smoking initiation.[8] Nicotine products are highly addictive and smokers find that quitting after a period of regular use is difficult despite known health benefits to quitting.
Tobacco products have been heavily marketed and targeted to some of the most vulnerable communities in San Francisco. This includes African-American, LGBT, lower income, and homeless populations. The sale and use of these products has been normalized for generations, leading to mass addiction. Despite being the only known product that if used as directed on the label is known to cause disease and death, tobacco is still sold in many locations and continues to contribute to considerable death and disability. Tobacco product marketing and the resulting use is a major source of health inequity in the country and in San Francisco. Use of tobacco products among Californians is associated with uninsurance and underinsurance, lower educational attainment, poverty, and among men from communities of color.
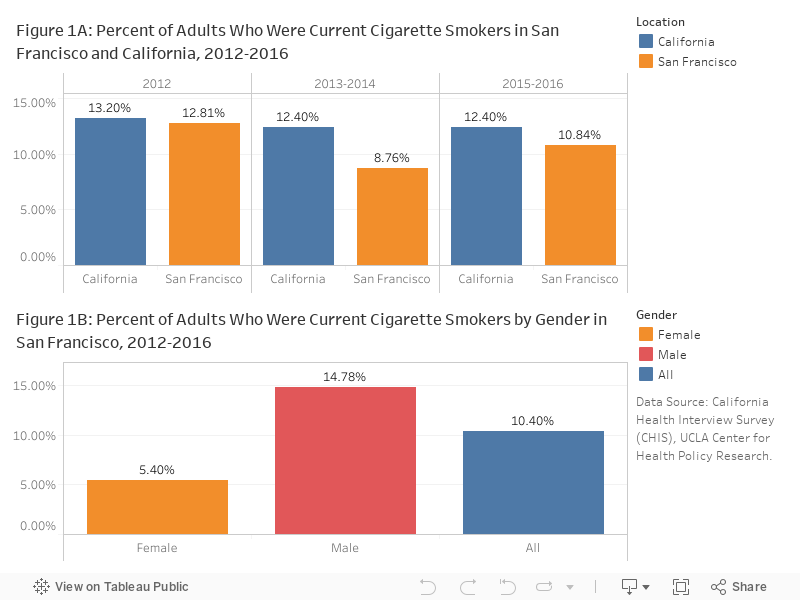
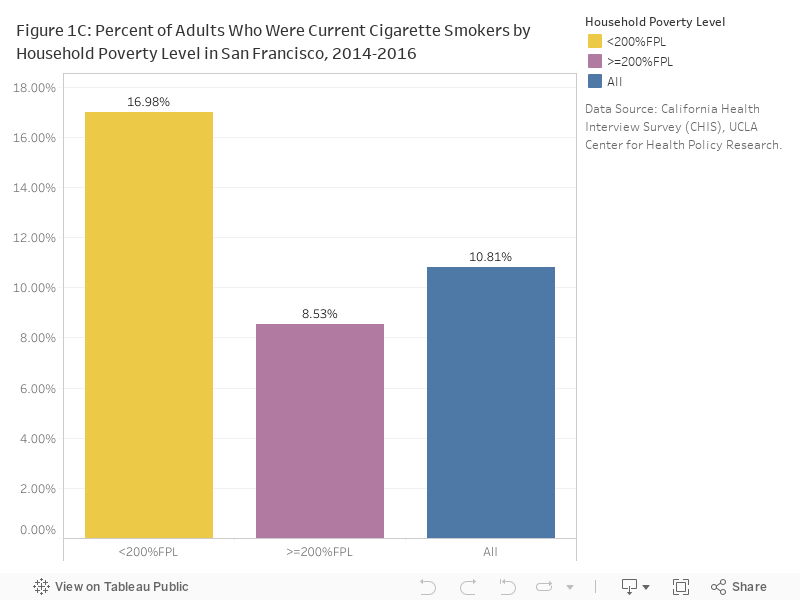
Smoking prevalence: In 2015-2016, 10.85% of adults in San Francisco reported they were current cigarette smokers, which slightly increased from 8.76% in 2013-2014; but the percentage was lower than California (12.40%) (Figure 1A). Men were almost 3 times more likely to smoke cigarette than women (Figure 1B) and the percentage among residents who lived below 200% of Federal Poverty Level was 2 times higher than residents who lived above 200% of Federal Poverty Level (Figure 1C).
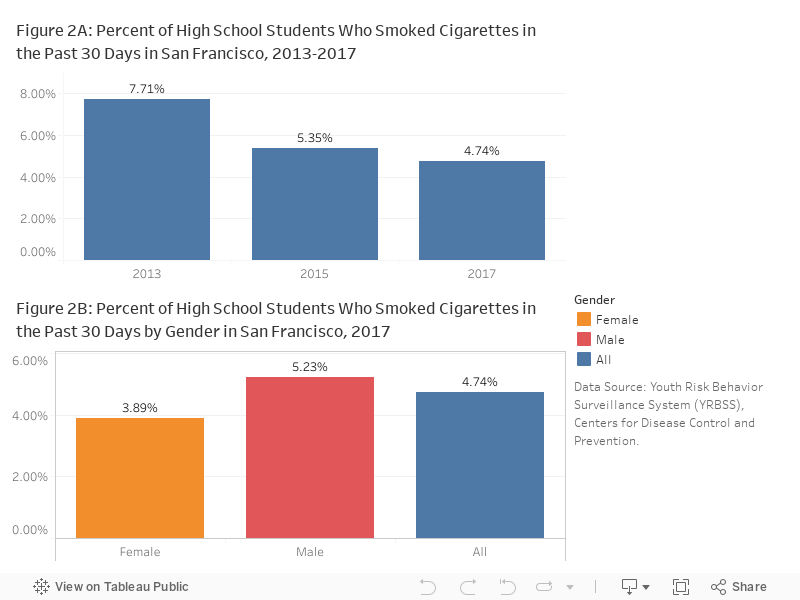
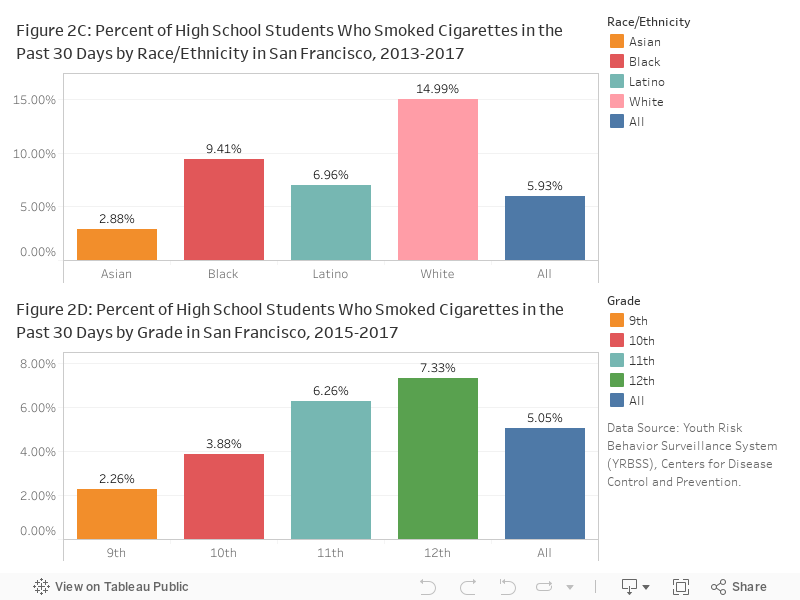
Smoking prevalence among high school students decreased between 2013-2017. 4.74% of the high school students said they smoked cigarettes in the past 30 days in 2017(Figure 2A). Similar to adults, male student were more likely to smoke cigarettes than female students (Figure 2B). The percentage was higher among White and Black students (15% and 9.4%) (Figure 2C) and it also increased along with age (Figure 2D).
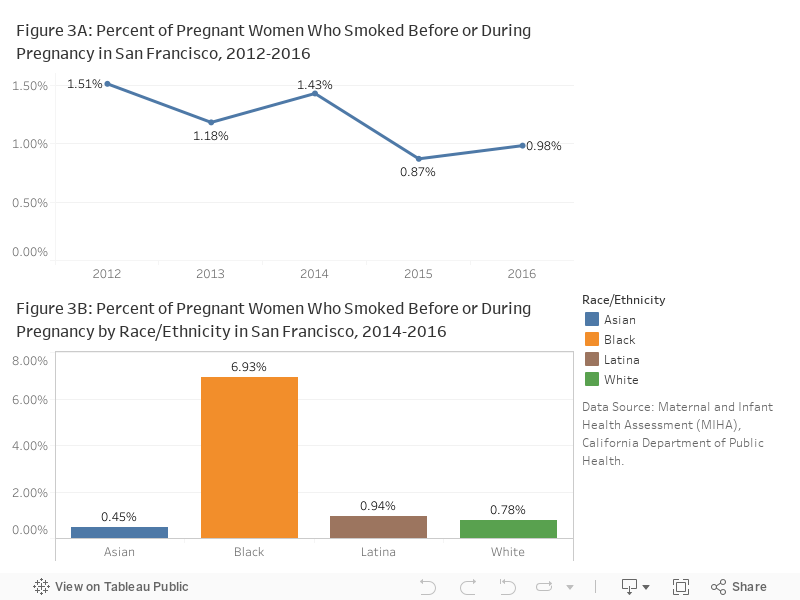
In 2016, 0.98% of new mothers in San Francisco reported smoking before or during pregnancy. The percentage has been dropping in the last 5 years from 1.51% in 2012 (Figure 3A). However, it was still 6-15 times higher among Black/African American women (6.83%) than all other races and ethnicities (Figure 3B).
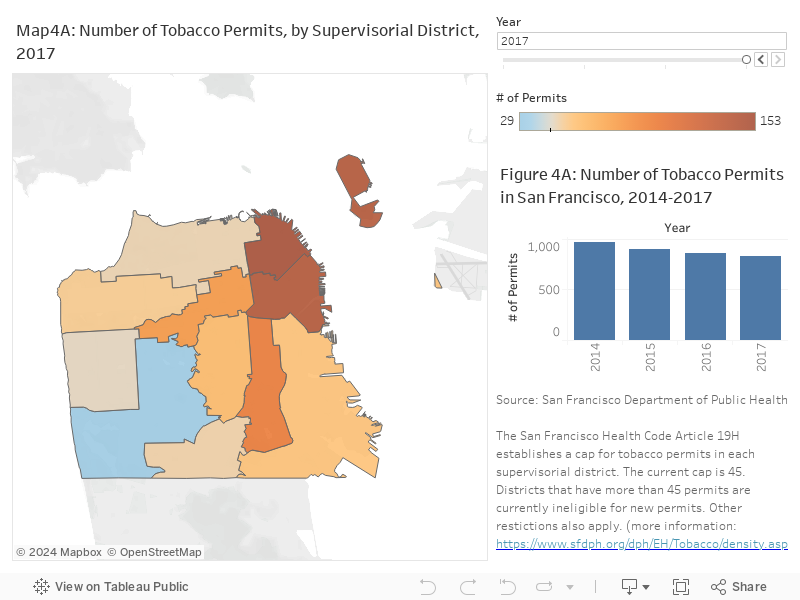
Tobacco permits and sales: Districts in San Francisco with higher concentrations of smokers, ethnic minorities, and youths are associated with a higher density of tobacco retailers, despite the fact that all the districts have approximately the same number of residents. These districts include historically ethnic neighborhoods such as the Mission, Tenderloin, Western Addition, Bayview Hunters Point, Excelsior, and Chinatown. Districts 3 (Chinatown), 6 (Tenderloin) which in 2017 included more than 140 tobacco retailers, while District 4 (The Sunset) had only 47 tobacco retailers (Map 4A).
Reducing tobacco retailer density and overall tobacco sales
Districts in San Francisco that are home to more people of color, low income people, and young people are also associated with a higher density of tobacco retailers and higher smoking rates [i.e., Mission, Tenderloin, Western Addition, Bayview Hunters Point, Excelsior, and Chinatown].
• In 2014, the San Francisco Board of Supervisors unanimously adopted the Tobacco Permit Density Reduction Ordinance, which limits new tobacco retailer permits near schools or other tobacco retailers.
Addressing e-cigarette use
“Vaping” is on the rise, especially among young people. In 2018 the number of 12th graders who reported e-cigarette use increased 78% from the prior year, causing the US Surgeon General to call for aggressive steps to curb the epidemic of teen nicotine use.23
San Francisco is leading the way with policies that directly address e-cigarettes’ health effects and popularity among minors.
• In 2014, San Francisco passed a law prohibiting use of electronic cigarettes wherever smoking of tobacco products is prohibited [SF Health Code Article 19N]
• In 2016, San Francisco raised the minimum age to purchase tobacco products from 18 to 21 [SF Health Code Article 19H]
• In 2018, San Francisco passed acomprehensive ban on flavored tobacco product sales, which includes flavored electronic tobacco pods. Proposition E, banned the sale of all flavored tobacco products, including e-liquids, menthol cigarettes, and flavored cigars. Tobacco companies designed the taste and packaging of flavored products to appeal to youth and have historically marketed menthol products specifically to the African American community. [SF Health Code Article 19Q]
CDPH Birth Statistical Master File, California Department of Public Health (CDPH).
CHIS California Health Interview Survey (CHIS), UCLA Center for Health Policy Research.
SFDPH Environmental Health Protection, Equity, and Sustainability Branch, San Francisco Department of Public Health (SFDPH).
YRBS Youth Risk Behavior Surveillance System (YRBSS), Centers for Disease Control and Prevention.
Survey sample sizes are not sufficiently large to create statically stable estimates for all age, gender, race and ethnicity, or poverty level stratifications.
Statistical instability: Statistically unstable estimates are not shown in this document. Statistical instability may arise from:
…few respondents to a survey,
…small population sizes, or
…small numbers of affected individuals.
Statistical instability indicates a lack of confidence in an estimates ability to accurately and reliably represent the population. Due to statistical instability, estimates are not available for all age, gender, ethnicity, or other groups.
[1] Ali H Mokdad, James S Marks, Donna F Stroup, and Julie L Gerberding. Actual causes of death in the united states, 2000. JAMA, 291:1238–1245, March 2004.
[2] California Tobacco Control Program California Department of Public Health. California tobacco facts and figures 2016. https://www.cdph.ca.gov/Programs/CCDPHP/DCDIC/CTCB/CDPH%20Document%20Library/ResearchandEvaluation/FactsandFigures/2016FactsFiguresWeb.pdf, 2016.
[3] Shannon M Farley, Hannah Seoh, Rachel Sacks, and Michael Johns. Teen use of flavored tobacco products in new york city. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco, 16:1518–1521, November 2014.
[4] Cristine D Delnevo, Daniel P Giovenco, Bridget K Ambrose, Catherine G Corey, and Kevin P Conway. Preference for flavoured cigar brands among youth, young adults and adults in the usa. Tobacco control, 24:389–394, July 2015.
[5] California Medical Association. Flavored and mentholated tobacco products: Enticing a new generation of users. http://www.cmanet.org/resource-library/detail/?item=flavored-and-mentholated-tobacco-products, 2016.
[6] Andrea C Villanti, Amanda L Johnson, Bridget K Ambrose, K Michael Cummings, Cassandra A Stanton, Shyanika W Rose, Shari P Feirman, Cindy Tworek, Allison M Glasser, Jennifer L Pearson, Amy M Cohn, Kevin P Conway, Raymond S Niaura, Maansi Bansal-Travers, and Andrew Hyland. Flavored tobacco product use in youth and adults: Findings from the first wave of the path study (2013-2014). American journal of preventive medicine, 53:139–151, August 2017.
[7] U.S. Department of Health and Human Services. Preventing tobacco use among youth and young adults: A report of the surgeon general. http://www.surgeongeneral.gov/library/reports/preventing-youth-tobacco-use/full-report.pdf, 2012.
[8] U.S. Department of Health and Human Services, “Substance abuse: Risk and protective factors.” Accessed July 2015. http://www.hhs.gov/ash/oah/adolescent-health-topics/substance-abuse/tobacco/risk-and-protective-factors.html#likelihood
[9] California Smokers’ Helpline, www.nobutts.org.
[10] Y. Chuang et al, “Effects of neighborhood socioeconomic status and convenience store concentration on individual-level smoking,” Journal of Epidemiology and Community Health, 59 (2009): 568–73.
[11] San Francisco Healthy Neighborhood Survey (2013).
[12] California Health Interview Survey (2011–12).
[13] San Francisco Unified School District (2014).
[14] W. Max et al, “The cost of smoking in California, 2009.” San Francisco: Institute for Health and Aging, University of California, San Francisco, 2014.
