Variables
- VEGETABLE AND FRUIT INTAKE
- DRINKING WATER INTAKE
- FAST FOOD INTAKE
- SODA INTAKE
- FOOD SECURITY
- FOOD ACCESS
Good nutrition means getting the right amount of nutrients from healthy foods, in the right combinations, on a daily basis. The right amount of nutrients varies from person to person depending on several factors, including age, sex, temperature, physical activity, stress, and health status [1]. For each kind of nutrient, the Food and Nutrition Board of the Institute of Medicine, National Academy of Sciences identifies a minimum daily amount to consume, sufficient to meet the nutrient requirement of nearly all (97%-98%) healthy people, and if appropriate, also a maximum daily amount to consume, above which excess consumption may cause adverse health effects [1]. Pregnancy can increase the minimum vitamin requirements [2]. Older age and chronic conditions, such as hypertension, can reduce the maximum safe limit for sodium (from 2300 mg in healthy younger adults to 1500 mg per day) [3].
According to national survey data, one third of US children and adults age 9 or older do not get enough vitamins. An estimated 31 percent do not meet minimum recommendations for vitamins A, B6, B12, C, D, E or Folate [4]. US adults do not meet recommended intakes for dietary fiber, calcium and potassium [5]. One third of US adults are inadequately hydrated, as evidenced by their highly concentrated urine [6, 7]. The low vitamin intake is attributed to low intake of vegetables and fruit (see Figure below). Highly concentrated urine reflects low water relative to salt.
National survey data further show that US Children and adults consume too much salt, solid fats, and added sugar [8-11] (see Figure below). Over 90 percent of the population consumes excess sodium relative to guidelines [12]. The recommended limit for added sugar intake is 5 teaspoons per day for women, 9 teaspoons per day for men, and 6 teaspoons per day for children [13, 14]. A typical American consumes vastly more sugar than the recommendation at almost 20 teaspoons of sugar per day [15].

To encourage people to eat more vitamins, the USDA MyPlate promotes a diet pattern where vegetables and fruits, which are rich in vitamins and minerals, take up half of the plate at each meal [16]. Adults who engage in less than 30 minutes of moderate physical activity per day should consume 2–3 cups of vegetables and 1.5–2.0 cups of fruit each day or 5 or more servings of vegetables and fruit daily [17]. USDA food programs mandate that child care centers and schools serve 5 servings of vegetables and fruit over the course of the day at breakfast, lunch and snack [18]. Drinking water with and between meals is recommended as a way to meet water requirements without added sugar, fat, or calories [19].
To support people to eat less salt and sugar, the 2015-2010 Dietary Guidelines recommend limiting consumption of foods prepared away from home, commercially processed, prepared or fast food, and sugary drinks [20]. Commercially processed or fast food is a leading source of sodium in the US diet [21]. Sugary drinks are a leading source of added sugar [22].
Good nutrition depends on food security: access, at all times, to enough nutritious food to support an active, healthy life for all people [23]. To achieve food security a person must have the ability to secure resources to purchase nutritious food on a consistent basis, obtain foods safely and conveniently, and prepare healthy meals. They must have knowledge of basic nutrition, safety and cooking [23]. Access to high energy, nutrient poor foods may lead to nutritional deficiency and overweight and obesity, and does not make someone food secure [24].The right to food is a human right recognized by international human rights law [25]. Access to sufficient, safe, acceptable, and affordable drinking water is also recognized as a human right [26].

In 2016, 87.7 percent (110.8 million) of U.S. households were food secure throughout 2016. Nationally, food insecurity is associated with low income and Black/African American race-ethnicity [27]. Risks of multiple vitamin deficiencies, inadequate hydration, and excess sugar and salt intake are significantly greater for lower income groups and Black/African Americans compared to higher income groups and non-Hispanic White Americans [4, 7].
It is a national priority to promote health and reduce chronic disease risk through the consumption of healthful food and drink [28]. Good nutrition is critical for growth, development, physical and cognitive function, reproduction, mental health, immunity, and long-term health [1, 29-34]. Hydration is associated with improved cognitive and physical performance and reduced risk of disease and death [35, 36].
Diets that are low in fruit and vegetables and drinking water and high in fat and salt and soda are associated with weight gain, obesity, high blood pressure, heart attack, stroke, diabetes, kidney disease, and cancer [37]. An estimated 45 percent of all heart disease, stroke, and type 2 diabetes deaths are associated with poor nutritional intake of 10 dietary factors (low intake of vegetables, fruits, seafood, whole grains, nuts/seeds, polyunsaturated fats and high intake of sodium, red meats, processed meats, sugary beverages)[38]; Heart disease and stroke are the first and fourth leading causes of death in the US and diabetes is the 7th [39].
Water intake below requirements results in dehydration. Dehydration significantly alters cellular metabolism and physiology. Over the short-term, it impairs physical and cognitive performance [35]. Over the longer term, it increases risks of morbidity, disability, and mortality from a wide variety of conditions [35, 36]. Dehydration significantly magnifies the risk of death within one year following hospitalization for respiratory illness, gastroenteritis, other gastrointestinal conditions, urinary system infections, cancer, sepsis, cardiac diagnoses, frailty, diabetes, and other metabolic disorders [36]. As dehydration is preventable and treatable, hospitalizations due to dehydration are tracked by the California Office of Statewide Health Planning and Development as an indicator of quality of services in the community [40].
Alleviating food insecurity and ensuring access to safe drinking water is essential to improving health outcomes and lowering health-related expenditures.
Do San Franciscans consume too little?
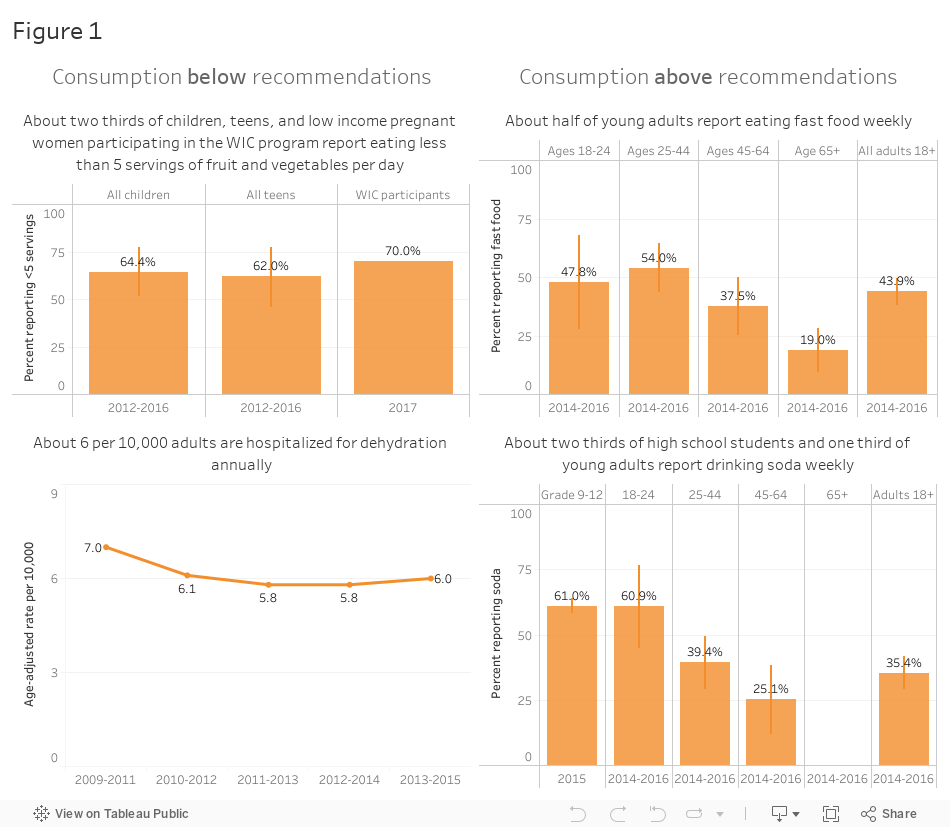
Local consumption of fruit and vegetables is below recommendations for the majority of children and at least 1 in 10 adults (see Figure 1). In 2012-2016, the California Health Interview Survey asked children and teens in San Francisco “Yesterday, how many servings of fruit, such as an apple or banana, did you eat?” AND “Yesterday, how many servings of vegetables, like corn, green beans, green salad, or other vegetables did you have?” About two thirds of San Francisco children and teens reported eating less than 5 servings of fruits and vegetables daily. In 2015, the BRFSS survey asked a similar question to adults in San Francisco; 14 percent of respondents reported eating vegetables less than one time per day [41]. In 2017, 70 percent of low income pregnant women participating in the Women Infants and Children (WIC) Eat SF program in San Francisco reported consuming fruit and vegetables less than 5 times per day [Personal communication, SFDPH Nutrition Services Director].
At least 1 in 10 San Franciscans do not meet the recommendation to drink water with and between meals. In 2013-2015, an estimated 16 percent of teens and adults in San Francisco reported drinking less than 3 glasses of water at school/work, home, and everywhere else in the past 24 hours [42]. In 2016, 614 people were hospitalized for “potentially preventable” dehydration in San Francisco [43].
Do San Franciscans consume too much?
Local consumption of fast food is in excess of recommendations. Over the past five years, just over 40 percent of San Franciscans reported eating fast food at least weekly (see Figure 1). Younger adults and males were over two times more likely to report eating a fast food meal at work, school, home, a restaurant, carryout or drive thru in the past 7 days [41]. In 2014-2016, 54 percent of adults between the ages 25 to 44 years reported eating fast food at least weekly compared to 19 percent of adults aged 65 or older. Half of the men who responded to the California Health Interview Survey reported eating fast food weekly, compared to 37 percent of the women surveyed [41].
Citywide, in 2014-2015, about two thirds of high school students and one third of young adults reported drinking at least one can, bottle or glass of soda (not counting diet soda) in the past 7 days (see Figure 1). Older adults were less likely to report weekly soda consumption than younger adults. In 2014-2015, soda consumption among adults age 25-44 years was not significantly different from soda consumption in 2011-2013 (42.0 percent) [41].
Among preschoolers, age 3, fruit and vegetable intake increases significantly more during the academic year for higher income children than lower income children [44]. Fruit and vegetable intake is expected to increase as children grow and become familiar with a variety of fruit and vegetables. Whereas the Veggie Meter score increased by an average of 69 points between Fall and Spring health screenings in 2016-2017 for higher income children, age 3, the Veggie Meter score decreased by an average of 6 points for lower income children of the same age. Mean changes in Veggie Meter score differed significantly by race-ethnicity, with mean change of +44 points for White children, compared to mean changes of 0, -17, and +25, for Asian, Latino and Black/African American children, respectively [44].
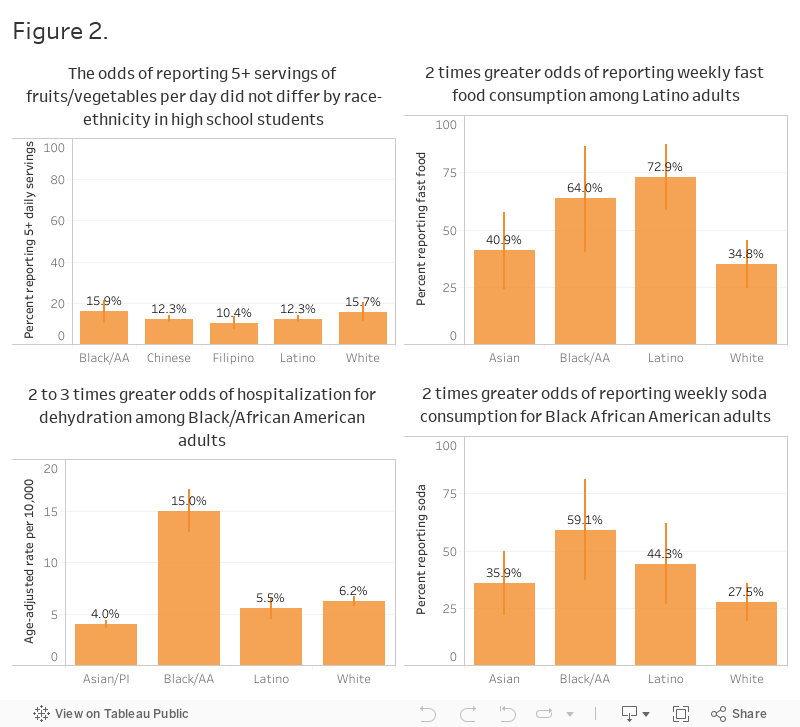
Among high school students, the odds of reporting 5 or more servings of fruit and vegetables per day does not vary by race-ethnicity (See Figure 2). In 2013-2017, 16 percent of Black/African American and White students and 12 percent of Chinese and Latino students reported eating 5 or more servings of fruit and vegetables per day.
Among adults, the odds of reporting fast food and soda and the likelihood of hospitalization for dehydration (low water intake) varies by race-ethnicity (See Figure 2). Two times more Latino adults reported eating fast food at least weekly than White adults. Two times more Black/African American adults reported soda intake than White adults. The odds of an emergency room visit for dehydration were higher for Black/African American adults than other race-ethnic groups.
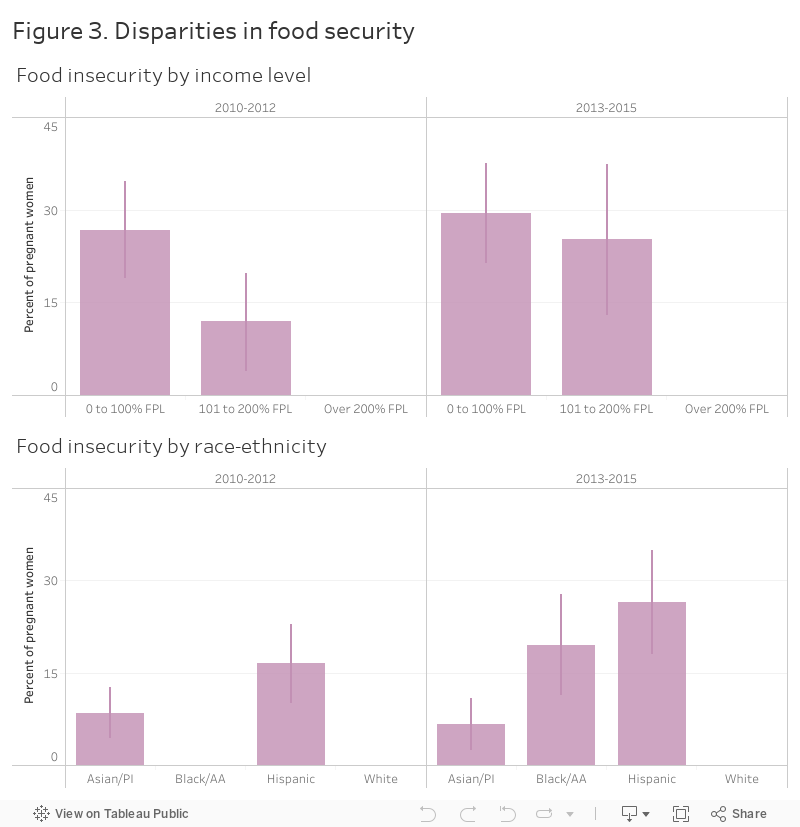
Food insecurity is prevalent among vulnerable groups in San Francisco, pregnant women, children, and older adults, and associated with socio-economic disparity.
In 2013-2015, over one quarter of pregnant women living in San Francisco with an income below 200 percent of the Federal Poverty Level reported food insecurity (See Figure 3). Food insecurity was reported by 20 percent of Black/African American pregnant women and 27 percent of Hispanic pregnant women. Between 2010 and 2015, food insecurity among pregnant women in San Francisco did not decrease, with trends suggesting worsening food insecurity for women with an income between 101-200 percent of the Federal Poverty Level and Hispanic women. In 2017, 72 percent of low income pregnant women who participated in the WIC Eat SF program reported food insecurity (WIC EAT SF program data, Personal communication, SFDPH Nutrition Services Director).
In 2016-2017, half of the students (53 percent) in the San Francisco Unified School District qualified for free or reduced-price meals [45]. The schools served over 35,000 free or reduced-price meals daily to children [45].
Figure 4 describes the number of food insecure adults and seniors who were eligible to receive home delivered meals, home delivered groceries or eating vouchers in San Francisco 2017-2018. Of 102,902 eligible individuals needing meals, only 34 percent received meals [46]. Food insecure homebound seniors, adults with disabilities, low income pregnant women and residents of single resident occupancy (SRO) hotels have unmet need. According to the Food Security Task Force, 80 percent of SRO residents, approximately 19,400 people, and 30,000 SSI recipients who are not eligible for CalFresh, are food insecure and at high nutritional risk [46].

Limited access to healthy food and drinking water
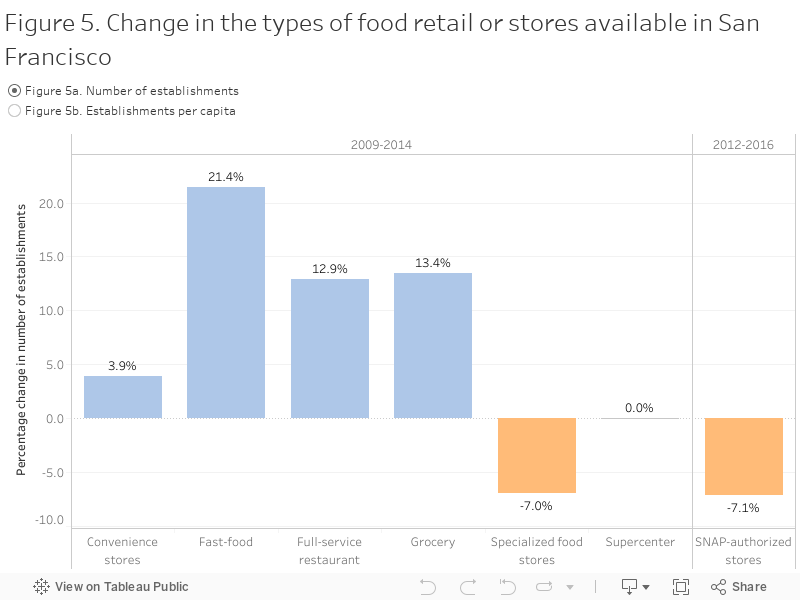
Consistent with nationwide norms to spend less time cooking and eat more meals away from home, access to ready-to-eat meals at fast food stores and full service restaurants increased in San Francisco between 2009 and 2014 (see Figure 5a). The number of fast food restaurants increased by 21 percent from 761 to 924. The number of full service restaurants increased by 13 percent from 1676 to 1893. In 2014, there were 1.1 fast food restaurants and 2.2 full service restaurants for every 1,000 people in San Francisco. Meanwhile, the number of vendors authorized to accept SNAP (food stamps) decreased by 7 percent. In 2016, 0.55 stores per 1,000 people accepted SNAP.
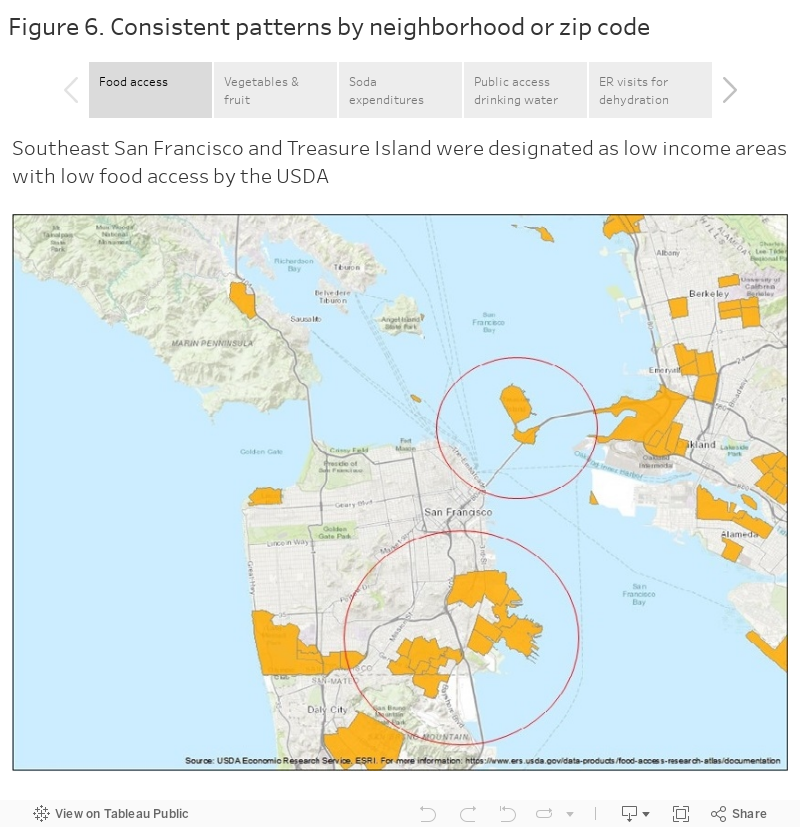
Available data suggest that the odds of not meeting dietary recommendations, not eating enough fruit and vegetables, drinking too little water, and drinking soda, differ by neighborhood. Furthermore, importantly, the pattern of differences across neighborhoods is similar across nutrition measures, suggesting that the neighborhoods that have low access to food are the same neighborhoods that purchase the fewest fruit and vegetables, purchase the most soda and experience the highest rates of emergency room hospitalizations for dehydration(See Figure 6).
The San Francisco Food Security Task Force (FSTF) advises the San Francisco Board of Supervisors on food security in San Francisco. Established in 2005 by the Board of Supervisors, the FSTF recommends citywide strategies, including legislative policies and budget proposals, to address hunger and increase food security in San Francisco. The FSTF tracks vital data on hunger and food security, including demographic information to understand the scope of need in general and for specific vulnerable subpopulations; data on utilization of federal food assistance programs such as CalFresh and school meals; and data onparticipation in nonprofit food and meal programs. The FSTF membership comprises representatives from 15 public and community – based entities in SF [46].
In 2013, the Board of Supervisors unanimously resolved to take steps to end hunger in San Francisco by 2020. In fiscal years 2017-2018 and 2018-2019, $10,665,000 million dollars were requested for San Francisco agencies to address local food insecurity. The San Francisco Department of Aging and Adult Services, Department of Public Health and Human Services Agency offered nutrition programs, healthy eating vouchers, and developed a SRO food security initiative. Specific FSTF aims for 2017-18 were to ensure that the waitlist for home delivered meals did not exceed 30 days, promote standardized food security screening in all nutrition and other programs serving individuals at risk for food insecurity, increase SSI/SSP payments for elderly, blind or disabled individuals, and estimate the cost of food insecurity to San Francisco [46].
CHIS California Health Interview Survey. http://askchis.ucla.edu
San Francisco Food Security Task Force Presentations
Neilsen Percent of Food-At-Home Expenditures
OSHPD Office of Statewide Health Planning and Development
SFDPH Child Care Health Program
WIC Program Eat SF WIC participant survey, 2017.
USDA Economic Research Service
YRBS Youth Risk Behavioral Surveillance System. http://www.cdc.gov/healthyyouth/data/yrbs/index.htm
Detailed dietary data, such as are available from the National Health and Nutrition Examination Survey (NHANES), are not available at the county level. For this reason, information is limited about the nutritional status, quantity and quality of dietary intake of San Franciscans. Self-reported servings of vegetable, fruit and water intake and food or beverage expenditure data are prone to measurement error and are not direct or sensitive measures of total energy intake, the various nutrients, or dietary pattern. No citywide-representative information is available about the usual daily consumption of added sugar, fat or salt intake. The number of self-reported servings are considered relative to national dietary guidelines, but are not direct measures of the adequacy of each individual’s diet relative to actual nutrient requirements. The meaning or adequacy of one cup of vegetables, for example, may be different for a small vs a large person, for a physically inactive person vs an athlete. The available dehydration measure is based on ICD10 codes, not direct biomarker assessment. The frequency of eating fast food underestimates the consumption of all commercially prepared food. Data are not available to describe dimensions of food security, access, acceptability and affordability across San Francisco neighborhoods, over time. The available data may be only be generalizable to selected populations, people willing to respond to surveys and/or participate in particular programs. The available local data are not directly comparable to the national NHANES data.
[1] “Nutrient Recommendations: Dietary Reference Intakes (DRI).” NIH Office of Dietary Supplements, U.S. Department of Health and Human Services, ods.od.nih.gov/Health_Information/Dietary_Reference_Intakes.aspx.
[2] Institute of Medicine. 2000. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. Washington, DC: The National Academies Press. https://doi.org/10.17226/9810.
[3] United States Food & Drug Administration. Lowering Salt in Your Diet. https://www.fda.gov/ForConsumers/ConsumerUpdates/ucm181577.htm
[4] Bird, Julia K., et al. “Risk of Deficiency in Multiple Concurrent Micronutrients in Children and Adults in the United States.” Nutrients Journal, MDPI, 24 June 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5537775/pdf/nutrients-09-00655.pdf.
[5] O’Neil CE, Keast DR, Fulgoni III VL, Nicklas TA. Food Sources of Energy and Nutrients among Adults in the US: NHANES 2003–2006. Nutrients. 2012 Dec; 4(12): 2097–2120. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3546624/#B17-nutrients-04-02097
[6] Chang T, Ravi N, Plegue MA, Sonneville KR. Inadequate Hydration, BMI, and Obesity Among US Adults: NHANES 2009–2012. The Annals of Family Medicine, Annals of Family Medicine, 2016, www.annfammed.org/content/14/4/320.full.
[7] Brooks, Carolyn J., et al. “Racial/Ethnic and Socioeconomic Disparities in Hydration Status Among Adults and the Role of Tap Water and Other Beverage Intake.” Advances in Pediatrics., U.S. National Library of Medicine, Sept. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5551608/.
[8] Krebs-Smith, Susan M., et al. “Americans Do Not Meet Federal Dietary Recommendations.” Advances in Pediatrics., U.S. National Library of Medicine, Oct. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2937576/.
[9] Agarwal S, Fulgoni VL 3rd, Spence L, Samuel P. Sodium intake status in United States and potential reduction modeling: an NHANES 2007-2010 analysis. Food Sci Nutr. 2015 Jun 9;3(6):577-85. doi: 10.1002/fsn3.248. eCollection 2015 Nov.
[10] Fulgoni VL 3rd, Agarwal S1, Spence L, Samuel P. Sodium intake in US ethnic subgroups and potential impact of a new sodium reduction technology: NHANES Dietary Modeling. Nutr J. 2014 Dec 18;13(1):120. doi: 10.1186/1475-2891-13-120.
[11] Powell, Elyse S., et al. “Added Sugars Intake across the Distribution of US Children and Adult Consumers: 1977-2012.” Advances in Pediatrics., U.S. National Library of Medicine, Oct. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC5039079/.
[12] Joyce Maalouf, MS, MPH,corresponding author Mary E. Cogswell, RN, DrPH, Janelle P. Gunn, RD, MPH, Christine J. Curtis, MBA, Donna Rhodes, RD, MS, Kathy Hoy, RD, EdD, Pamela Pehrsson, PhD, Melissa Nickle, MPH, and Robert Merritt, MA. Monitoring the Sodium Content of Restaurant Foods: Public Health Challenges and Opportunities. Am J Public Health. 2013 September; 103(9): e21–e30.
[13] Johnson RK, Appel LJ, Brands M, Howard BV, Lefevre M, Lustig RH, Sacks F, Steffen LM, Wylie-Rosett J; American Heart Association Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism and the Council on Epidemiology and Prevention. Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation. 2009 Sep 15;120(11):1011-20. doi: 10.1161/CIRCULATIONAHA.109.192627. Epub 2009 Aug 24.
[14] Vos MB, Kaar JL, Welsh JA, Van Horn LV, Feig DI, Anderson CAM, Patel MJ, Cruz Munos J, Krebs NF, Xanthakos SA, Johnson RK; American Heart Association Nutrition Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Functional Genomics and Translational Biology; and Council on Hypertension. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement From the American Heart Association. Circulation. 2017 May 9;135(19):e1017-e1034. doi: 10.1161/CIR.0000000000000439. Epub 2016 Aug 22.
[15] Ervin RB, Ogden CL. Consumption of added sugars among U.S. adults, 2005-2010. NCHS Data Brief. 2013 May;(122):1-8.
[16] http://www.choosemyplate.gov/printpages/MyPlateFoodGroups/Fruits/food-groups.fruits-amount.pdf and http://www.choosemyplate.gov/printpages/MyPlateFoodGroups/Vegetables/food-groups.vegetables-amount.pdf
[17] Moore LV, Thompson FE. Adults Meeting Fruit and Vegetable Intake Recommendations — United States, 2013. Morbidity and Mortality Weekly Report (MMWR). July 10, 2015 / 64(26);709-713 https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6426a1.htm
[18] Updated Child and Adult Care Food Program Meal Patterns: Child and Adult Meals. United States Department of Agriculture, 25 Apr. 2016, fns-prod.azureedge.net/sites/default/files/cacfp/CACFP_MealBP.pdf.
[19] USDA ChooseMyPlate.gov 10 Tips: Make Better Beverage Choices. https://www.choosemyplate.gov/ten-tips-make-better-beverage-choices
[20] https://health.gov/dietaryguidelines/2015/guidelines/chapter-2/a-closer-look-at-current-intakes-and-recommended-shifts/
[21] Harnack LJ, Cogswell ME, Shikany JM, Gardner CD, Gillespie C, Loria CM, Zhou X, Yuan K, Steffen LM. Sources of Sodium in US Adults From 3 Geographic Regions. Circulation. 2017 May 9;135(19):1775-1783. doi: 10.1161/CIRCULATIONAHA.116.024446.
[22] Powell ES, Smith-Taillie LP, Popkin BM. Added Sugars Intake Across the Distribution of US Children and Adult Consumers: 1977-2012. J Acad Nutr Diet. 2016 Oct;116(10):1543-1550.e1. doi: 10.1016/j.jand.2016.06.003. Epub 2016 Aug 1.
[23] San Francisco Food Security Task Force. Assessment of Food Security in San Francisco, 2013. https://www.sfdph.org/dph/files/sfchip/fstf-assessmentoffoodsecurityinsf-2013.pdf
[24] Seligman HK, Laraia BA, Kushel MB. Food Insecurity Is Associated with Chronic Disease among Low-Income NHANES Participants. J Nutr. 2010 Feb; 140(2): 304–310.
[25] Office of the High Commissioner for Human Rights. United Nations Human Rights. The Right to Adequate Food. Fact Sheet No 34. https://www.ohchr.org/Documents/Publications/FactSheet34en.pdf
[26] de Albuquerque, Catarina (2014). Realising the human rights to water and sanitation: A Handbook by the UN Special Rapporteur (PDF). Portugal: United Nations. pp. “Introduction”.
[27] Pruitt, Sandi L., et al. “Preventing Chronic Disease.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 13 Oct. 2016, www.cdc.gov/pcd/issues/2016/16_0103.htm.
[28] https://www.healthypeople.gov/2020/topics-objectives/topic/nutrition-and-weight-status
[29] http://www.who.int/maternal_child_adolescent/documents/chs_cah_99_3/en/
[30] development https://www.unicef.org/nutrition/index_role.html
[31] https://khni.kerry.com/wp-content/uploads/2017/09/12988_KHNI_Sept_White_Paper_Nutrition_support_youth_9.21.17_Final.pdf
[32] brain https://www.nature.com/articles/s41538-017-0008-y
[33] reproduction https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4772050/
[34] aging https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4767865/
http://www.nap.edu/read/10925/chapter/1
[35] Institute of Medicine. 2005. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate.
[36] Warren JL, Bacon WE, Harris T, McBean AM, Foley DJ, Phillips C. The burden and outcomes associated with dehydration among US elderly, 1991. Am J Public Health. 1994 Aug;84(8):1265-9.
[37] WHO technical staff. Increasing fruit and vegetable consumption to reduce the risk of noncommunicable diseases, Biological, behavioural and contextual rationale. September 2014
http://www.who.int/elena/titles/bbc/fruit_vegetables_ncds/en/
[38] NIH. How dietary factors influence disease risk. https://www.nih.gov/news-events/nih-research-matters/how-dietary-factors-influence-disease-risk
[39] CDC, National Center for Health Statistics. Leading causes of death. Accessed 8-23-2018. https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
[40] Let’s get healthy California. https://letsgethealthy.ca.gov/goals/redesigning-the-health-system/reducing-preventable-hospitalizations/
[41] CDC. BRFSS Prevalence & Trends Data: Explore by Topic. https://nccd.cdc.gov/BRFSSPrevalence/rdPage.aspx?rdReport=DPH_BRFSS.ExploreByTopic&irbLocationType=StatesAndMMSA&islClass=CLASS06&islTopic=TOPIC60&islYear=2015&rdRnd=67664
[42] AskCHIS. Number of glasses of water drank yesterday. Source: 2013, 2014, 2015 California Health Interview Survey. Accessed 8-23-2018.
[43] OSHPD. Rates of Preventable Hospitalizations for Selected Medical Conditions by County (LGHC Indicator).
https://data.chhs.ca.gov/dataset/rates-of-preventable-hospitalizations-for-selected-medical-conditions-by-county
[44] SFDPH Child Care Health Program. 2016‐2017 Change in Fruit & Vegetable. Intake https://www.sfdph.org/dph/files/MCHdocs/Epi/Data-Table-Early-Childhood-Change-in-Fruit-and-Vegetable-Intake-2016-2017.pdf
[45] SFUSD Student Nutrition Services. San Francisco Unified School District, Food Security Task Force September 6, 2017 meeting presentation. https://www.sfdph.org/dph/files/mtgsGrps/FoodSecTaskFrc/docs/SNS_Food-Security-TF_Sep-2017.pdf
[46] San Francisco Food Security Task Force FY 2017-18 & FY 2019-20 Funding Request.
https://www.sfdph.org/dph/files/mtgsGrps/FoodSecTaskFrc/docs/FSTF-Budget-Request-FY-18-19.pdf
Accessed 8-24-2018.
